Say Goodbye to Painful Bowel Movements with SurgiPartner Advanced Fissure
Experience Gentle, Painless Healing with Laser Precision Care
Book Free Consultation
Fissure Treatment in Hyderabad — Laser Fissurectomy
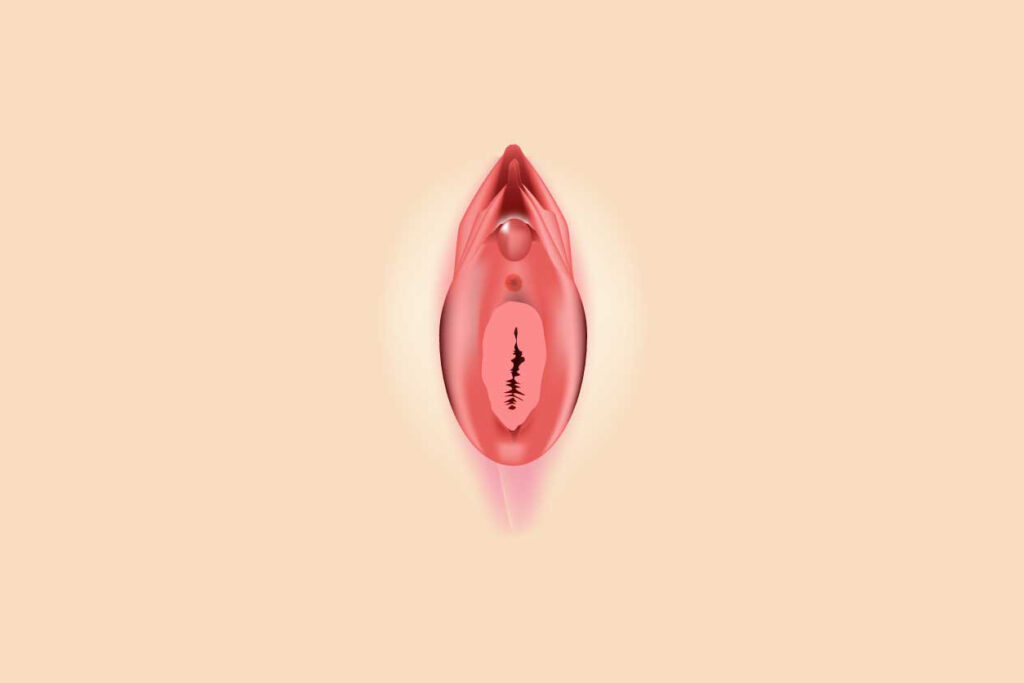
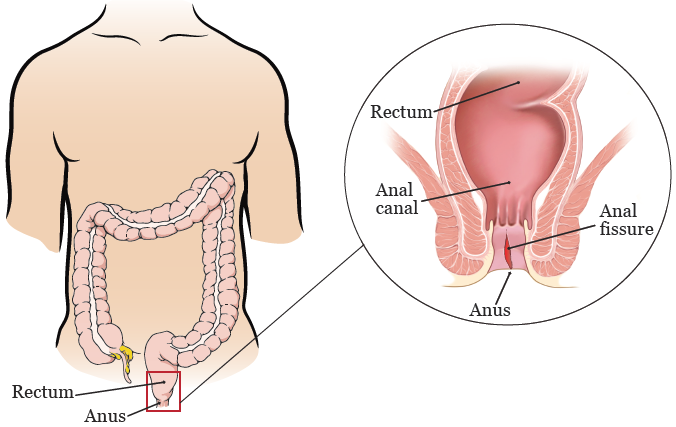
An anal fissure is a small tear, crack, or ulcer in the lining (anoderm) of the anal canal — one of the most painful anorectal conditions, causing severe tearing or burning pain during and after defecation that can persist for hours. Despite causing intense discomfort, many patients in Hyderabad delay seeking medical help for months due to embarrassment. Modern fissure treatment — including laser fissurectomy and lateral internal sphincterotomy (LIS) — is safe, effective, and highly successful. SurgiPartner connects patients in Hyderabad with colorectal specialists for confidential, effective fissure treatment.
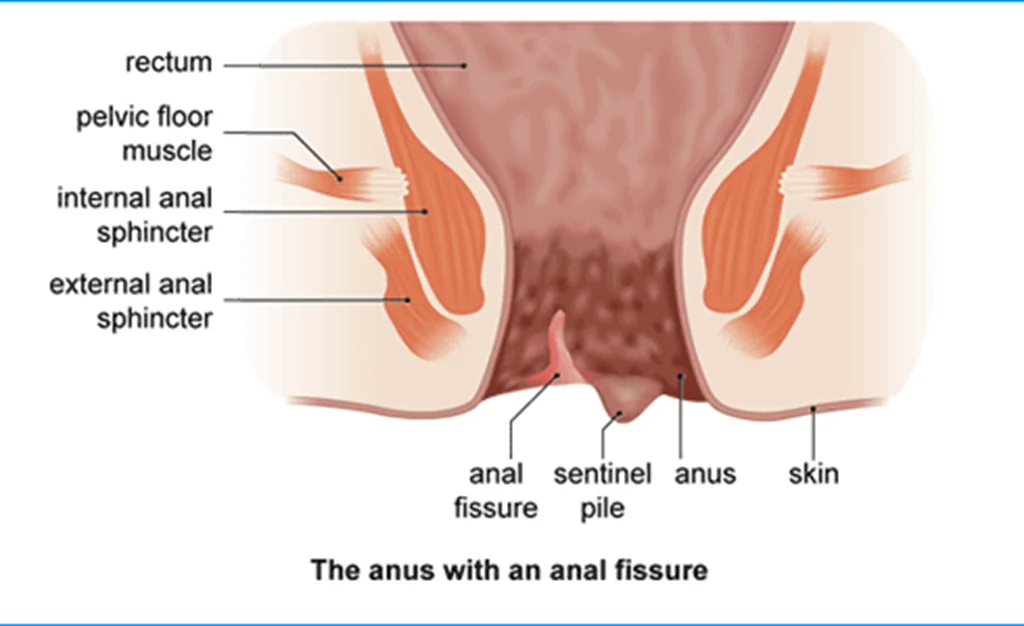
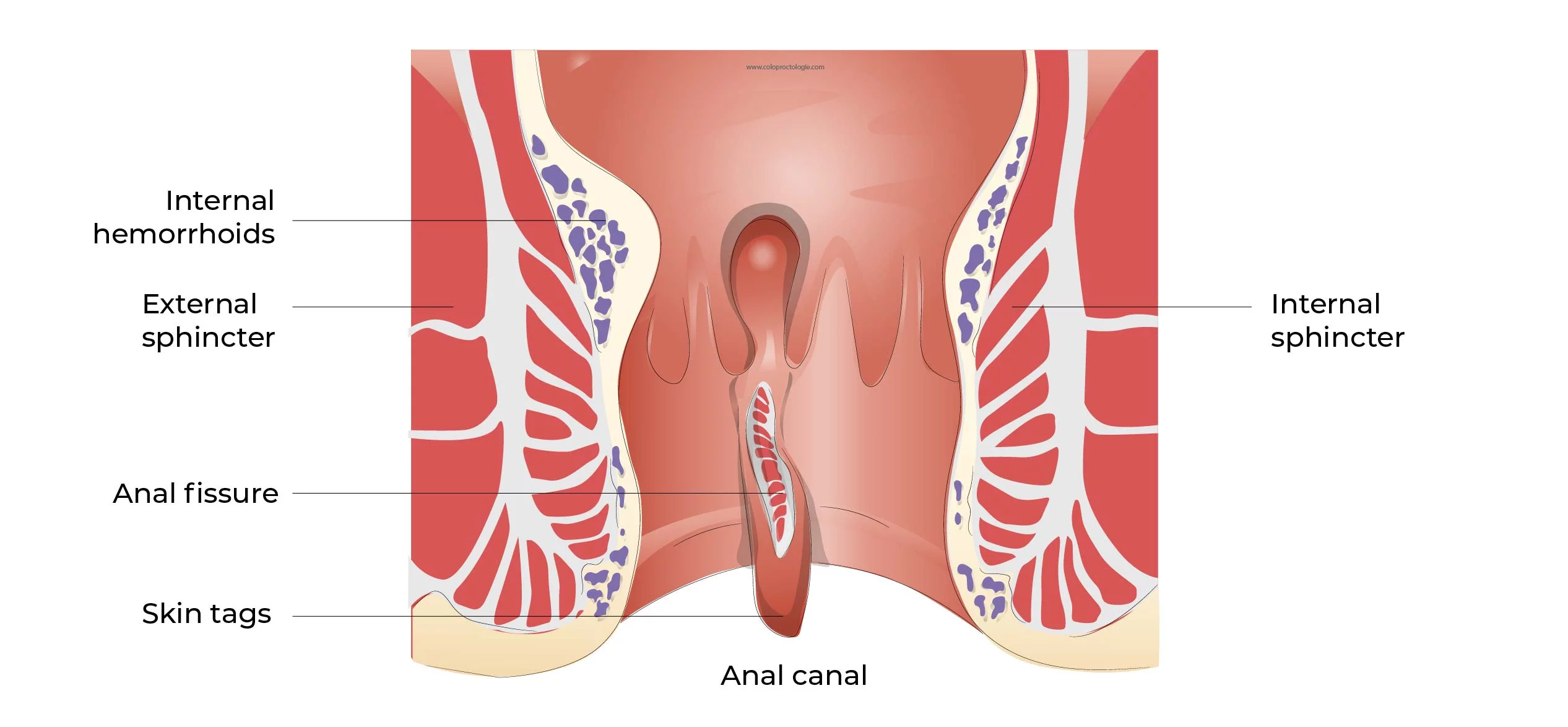
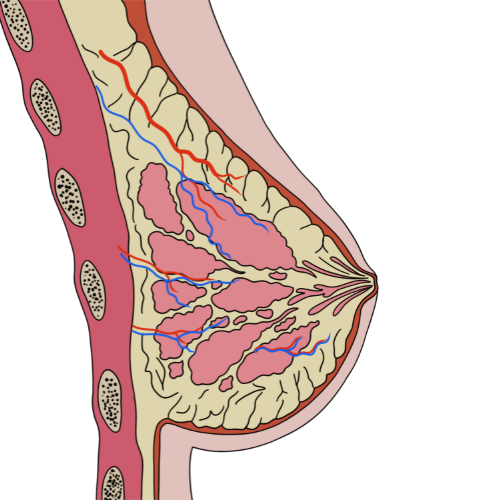
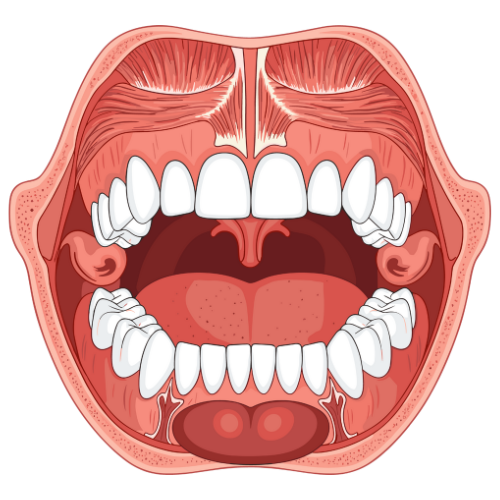
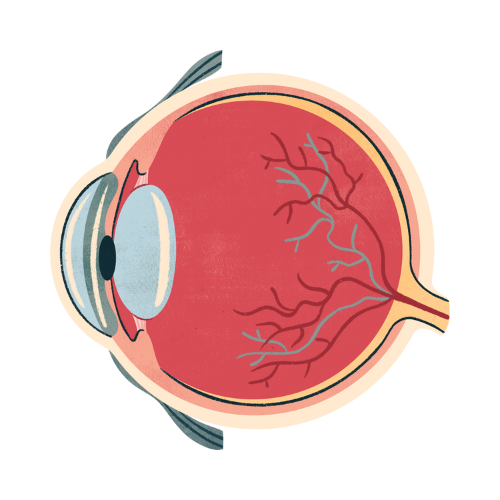
Anatomy — Why Anal Fissures Are So Painful
The anal canal is approximately 4cm long, bounded above by the dentate line and below by the anal verge. The lower anal canal (below the dentate line) is richly supplied by somatic pain fibres — making any breach of this lining exquisitely painful. A fissure in this location causes direct mucosal pain, and by exposing the underlying internal anal sphincter, triggers the vicious cycle of fissure pathophysiology: the fissure causes pain → pain triggers reflex internal sphincter spasm → sphincter spasm reduces blood supply to the posterior anal commissure (where 90% of fissures occur) → ischaemia impairs healing → the fissure persists and becomes chronic.
Acute vs Chronic Anal Fissure
| Feature | Acute Fissure | Chronic Fissure |
|---|---|---|
| Duration | <6 weeks | >6 weeks |
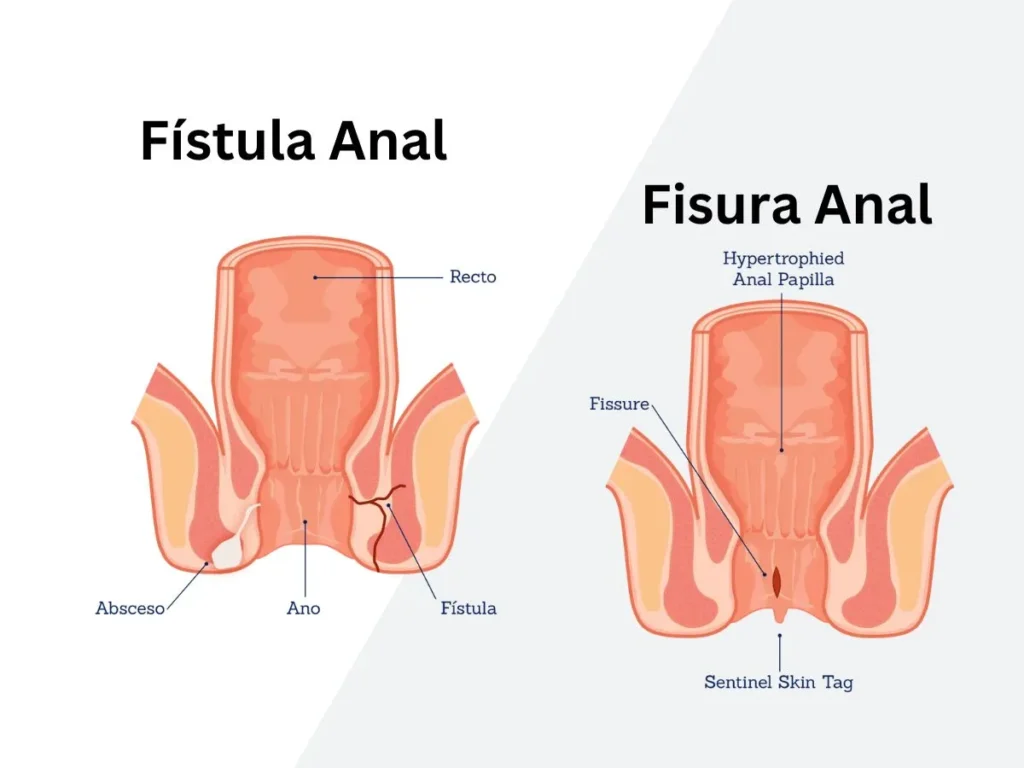
| Appearance on examination | Fresh mucosal tear with no fibrosis; clean edges; bleeds easily; may have sentinel pile (skin tag) externally | White fibrotic base with exposed white horizontal fibres of internal sphincter; sentinel pile externally; hypertrophied anal papilla internally; classic triad |
| Healing with conservative Rx | 50–80% heal with conservative management | <20% heal with conservative management; usually requires intervention |
| Treatment approach | Conservative first — diet, sitz baths, topical agents | Topical GTN or diltiazem → Botox if fails → LIS or laser surgery |
Causes and Predisposing Factors
- Constipation and hard stools — the most common precipitant; passage of a hard, large-calibre stool tears the anal mucosa
- Diarrhoea — particularly frequent, acidic diarrhoea; less common cause but well recognised
- Anal hypertonia — elevated resting internal anal sphincter pressure is the key perpetuating factor; explains the predominance of posterior midline fissures (the poorest blood supply point)
- Childbirth trauma — obstetric injury; anterior fissures in women are more common after delivery
- Inflammatory bowel disease — Crohn’s disease causes multiple, deep, irregularly placed fissures; treated differently from idiopathic fissure
- Sexually transmitted infections — herpes simplex, syphilis, and HIV can cause atypical anal ulceration mimicking fissure
Treatment Options — Stepwise Approach
Step 1: Conservative Management (All Acute Fissures)
Dietary modification — high-fibre diet (30g/day); 2.5–3 litres of fluid daily; psyllium husk (isabgol) 2 tablespoons daily in water. Sitz baths — warm water soaks for 10–15 minutes after each bowel movement; relieves sphincter spasm and improves perianal blood flow. Topical lignocaine gel or cream — applied 15–20 minutes before defecation to provide local anaesthetic relief; does not treat the underlying fissure but reduces the pain-spasm cycle. Stool softeners — lactulose, liquid paraffin, or macrogol reduce stool hardness and anal trauma during defecation.
Step 2: Topical Chemical Sphincterotomy
Glyceryl trinitrate (GTN) 0.2–0.5% ointment — applied twice daily to the perianal skin and anal canal; causes smooth muscle relaxation of the internal sphincter through nitric oxide donation; reduces resting anal pressure and improves blood flow; heals 50–60% of chronic fissures at 8 weeks. Side effect: headache (common, limits compliance). Topical diltiazem 2% ointment — calcium channel blocker; similar efficacy to GTN; fewer headaches; preferred when GTN headaches limit compliance. Both are applied for 8–12 weeks as a treatment course.
Step 3: Botulinum Toxin Injection (Botox)
Botulinum toxin type A (20–30 units) is injected into the internal anal sphincter on each side — typically under local anaesthesia as an outpatient procedure. Causes chemical denervation and temporary relaxation of the internal sphincter for 3–6 months — allowing fissure healing in 50–80% of cases. Complications: transient faecal incontinence (5–10%, almost always temporary); incomplete response (repeat injection possible). More effective than topical agents for chronic fissures that have failed 8 weeks of conservative/topical treatment.
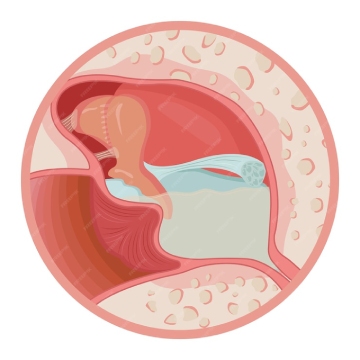
Step 4: Lateral Internal Sphincterotomy (LIS) – Surgical Gold Standard
LIS is the definitive surgical treatment for chronic anal fissure that has failed non-operative management — achieving healing in 90–98% of patients. The procedure involves carefully dividing the lower fibres of the internal anal sphincter (typically 30–40% of its length) at the 3 o’clock (lateral) position — completely separate from the fissure — under general or spinal anaesthesia. Dividing the sphincter at the lateral position reduces the resting sphincter pressure, breaking the ischaemic cycle and allowing the fissure to heal.
Duration: 15–20 minutes; day-care procedure. The fissure site itself is not touched (in contrast to open fissurectomy). Main concern: risk of faecal incontinence from excessive sphincter division — minimised by limiting division to the lower 30–40% of the sphincter using the fissure apex as the landmark. Incontinence rates with correctly performed LIS: minor gas incontinence 5–10% (usually temporary); liquid or solid incontinence <1%.
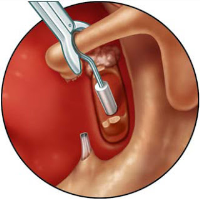
Laser Fissurectomy – Modern Minimally Invasive Option
Laser fissurectomy uses a diode laser to ablate the chronic fibrotic fissure base and sentinel pile, stimulating fresh tissue healing without the need for sphincterotomy. Suitable for fissures where sphincter division risk is a concern (anterior fissures, elderly patients, patients with pre-existing incontinence, women after childbirth). Combined with Botox injection to address the sphincter hypertonia component. Less data than LIS; healing rates approximately 75–85% at 6 months.
Frequently Asked Questions — Fissure Treatment Hyderabad
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing comfort, care, and modern medical excellence. Our advanced Laser Fissure Treatment provides instant relief from pain and bleeding with faster recovery and no hospital stay.
01.
Expert Proctologists & Surgeons
Our team of specialists has years of experience in treating anal fissures and other anorectal conditions with outstanding success rates.
02.
Advanced Laser Technology
We use precision laser techniques that promote rapid healing, minimal pain, and virtually no bleeding during or after treatment.
03.
Personalized Treatment Plans
Every fissure case is different we create a tailored treatment plan focused on your comfort, quick healing, and long-term relief.
04.
Pain-Free & Quick Recovery
Most patients are treated on a day-care basis and return to normal routines within 24 hours with continuous post-care support.
Book Your Consultation
Take the first step toward pain-free healing with SurgiPartner Advanced Laser Fissure Treatment. Our specialists are here to provide safe, effective, and compassionate care.
Healing made simple and painless – that’s the SurgiPartner promise.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.