Pelvic & Abdominal Pain Treatment in Hyderabad
Chronic pelvic and abdominal pain is one of the most debilitating and misunderstood pain conditions — affecting an estimated 15–25% of women and 10–12% of men at some point in their lives. It is defined as pain in the pelvic or lower abdominal region persisting for 6 months or longer, often significantly impacting quality of life, sexual function, work capacity, and emotional wellbeing. Many patients spend years cycling through investigations and specialist consultations without relief. SurgiPartner’s pain management specialists in Hyderabad offer a comprehensive, interventional approach — targeting the specific nerve pathways responsible for pelvic and abdominal pain transmission to achieve lasting relief where medications have failed.
Understanding Chronic Pelvic and Abdominal Pain — The Complexity
Chronic pelvic pain (CPP) is not a single disease — it is a syndrome with multiple potential contributing mechanisms operating simultaneously. Understanding why pelvic pain is so complex requires appreciating the dense and overlapping innervation of the pelvis:
- Sympathetic nervous system — the superior hypogastric plexus (T10–L2 origin) transmits sympathetic pain signals from the uterus, ovaries, bladder, distal colon, rectum, and prostate. The inferior hypogastric plexus coordinates pelvic organ visceral sensation.
- Parasympathetic nervous system — pelvic splanchnic nerves (S2–S4) carry parasympathetic and some sensory fibres from the lower pelvis and perineum
- Somatic nervous system — the pudendal nerve (S2–S4) supplies the perineum, external genitalia, external anal and urethral sphincters; pudendal neuralgia is a recognised cause of chronic pelvic pain, particularly in women and cyclists
- Central sensitisation — in long-standing CPP, the spinal cord and brain undergo neuroplastic changes that amplify pain signals — explaining why patients continue to experience severe pain even when the original peripheral trigger has been resolved
Causes of Chronic Pelvic and Abdominal Pain
Gynaecological Causes (Women)
- Endometriosis — the most common gynaecological cause of CPP; endometrial-like tissue implants in the pelvis causing cyclic and non-cyclic pain, dyspareunia, dyschezia, and infertility
- Adenomyosis — endometrial tissue within the uterine muscle; severe dysmenorrhoea and heavy periods
- Pelvic inflammatory disease (PID) — chronic PID following inadequately treated sexually transmitted infection leaves fibrotic adhesions and nerve sensitisation
- Ovarian remnant syndrome — residual ovarian tissue after oophorectomy producing cyclic pain
- Pelvic congestion syndrome — pelvic varicose veins causing a dull, aching pelvic heaviness worsened by prolonged standing, sexual intercourse, and menstruation
Urological Causes
- Interstitial cystitis / bladder pain syndrome (IC/BPS) — chronic bladder inflammation without infection causing severe urinary frequency, urgency, and suprapubic pain
- Chronic prostatitis / chronic pelvic pain syndrome (CPPS) in men — the most common cause of CPP in men under 50; pelvic, perineal, and testicular pain with variable urinary and sexual dysfunction
Gastrointestinal Causes
- Irritable bowel syndrome (IBS) — functional gut disorder with abdominal cramping, bloating, and altered bowel habit; visceral hypersensitivity is the central mechanism
- Chronic mesenteric ischaemia — abdominal pain 20–60 minutes after eating; weight loss; vascular assessment essential
- Abdominal adhesion pain — fibrotic bands from previous surgery causing intermittent obstruction and traction pain
Musculoskeletal and Neurological Causes
- Myofascial pelvic floor dysfunction — hypertonic (overactive) pelvic floor muscles generating referred pain throughout the pelvis, perineum, and abdomen
- Pudendal neuralgia — entrapment or injury of the pudendal nerve causing severe burning, shooting perineal pain, often exacerbated by sitting; worse in cyclists, women after childbirth, patients after pelvic surgery
- Iliohypogastric/ilioinguinal nerve entrapment — post-surgical (particularly after hernia repair or caesarean section) causing burning pain in the inguinal region and lower abdomen
- Abdominal cutaneous nerve entrapment syndrome (ACNES) — entrapment of intercostal nerve endings in the rectus abdominis muscle causing localised abdominal pain; often misdiagnosed as gynaecological or gastroenterological pathology
Diagnosis — A Systematic Approach to Chronic Pelvic Pain
The diagnostic process for CPP requires thorough evaluation across multiple specialties. At SurgiPartner’s pain management centres in Hyderabad, the assessment protocol includes:
| Investigation | Purpose |
|---|---|
| Detailed pain history | Duration, character (burning, aching, cramping, stabbing), location, radiation pattern, provocative and relieving factors, menstrual cycle relationship, bowel/bladder association, sexual activity impact, psychosocial history |
| Pelvic examination | Identify gynaecological pathology; assess pelvic floor tone and trigger points; localise pudendal nerve tenderness; assess for ACNES using Carnett's test |
| Ultrasound pelvis (TVS) | Identify endometriomas, fibroids, ovarian pathology, pelvic varicosities, adenomyosis features |
| MRI pelvis with contrast | Comprehensive pelvic organ assessment; deep infiltrating endometriosis mapping; pelvic floor anatomy; pudendal nerve course |
| Laparoscopy | Gold standard for endometriosis diagnosis and staging; allows simultaneous surgical treatment of endometriotic deposits |
| Diagnostic nerve blocks | Superior hypogastric plexus block or pudendal nerve block as diagnostic and therapeutic procedures — significant pain relief confirms the nerve pathway as the source |
| Urodynamics + cystoscopy | Assess IC/BPS; exclude malignancy; evaluate bladder capacity under anaesthesia (hydrodistension) |
| Psychological assessment | Screen for depression, anxiety, PTSD, somatisation — central sensitisation components that significantly affect treatment response |
Interventional Pain Management — Targeting Pelvic Pain Pathways
Superior Hypogastric Plexus Block (SHPB)
The superior hypogastric plexus is a sympathetic nerve network situated in the retroperitoneum at the level of the L5–S1 intervertebral disc, anterior to the aortic bifurcation. It transmits pain signals from most pelvic viscera — making it an ideal target for interventional treatment of visceral pelvic pain from endometriosis, chronic pelvic inflammatory disease, interstitial cystitis, and cancer-related pelvic pain.
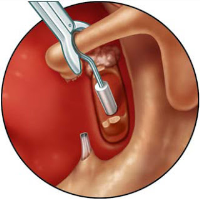
Technique: Performed under fluoroscopic (X-ray) or CT guidance with the patient prone; two needles are advanced to the retroperitoneal space at L5–S1; contrast is injected to confirm position; local anaesthetic (diagnostic block) or neurolytic agent (absolute alcohol or phenol for permanent relief in cancer pain) is injected. Duration of diagnostic block: 4–8 hours. Duration of benefit after neurolysis: weeks to months. Studies show 70–80% of patients with pelvic visceral pain achieve significant relief after SHPB.
Inferior Hypogastric Plexus Block
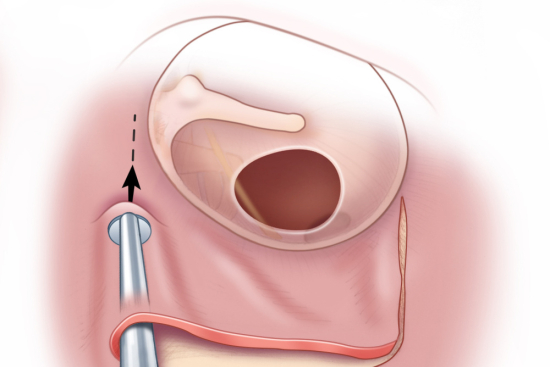
Targets the inferior hypogastric plexus (pelvic plexus) — relevant for perineal, rectal, bladder neck, and lower pelvic pain. Performed transvaginally (women) or transperineally under ultrasound guidance.
Pudendal Nerve Block
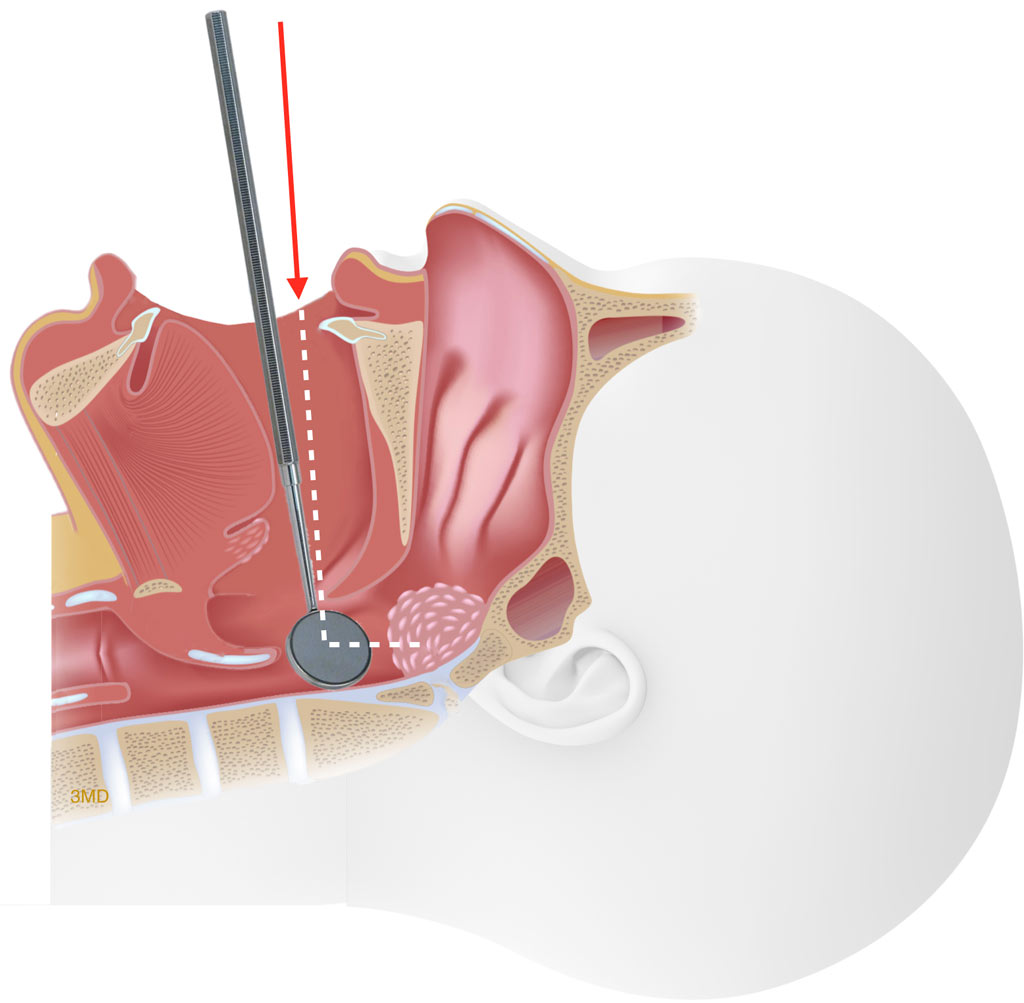
The pudendal nerve carries sensory fibres from the perineum, external genitalia, and anus. Pudendal nerve block is both diagnostic (confirming pudendal neuralgia as the pain source) and therapeutic. Performed under ultrasound or fluoroscopic guidance targeting the Alcock’s canal (where the nerve runs medial to the ischial spine). A combination of local anaesthetic and corticosteroid is injected. Significant pain relief after pudendal block confirms the diagnosis and guides further management — including pulsed radiofrequency ablation (PRF) of the pudendal nerve for sustained relief.
Pulsed Radiofrequency (PRF) Neuromodulation
PRF delivers short bursts of radiofrequency energy to the target nerve — causing long-lasting neuromodulation (altered nerve function reducing pain transmission) without the tissue destruction of continuous RF ablation. PRF of the superior hypogastric plexus, pudendal nerve, and sacral nerve roots (S2–S4) provides sustained pain relief for 3–12 months and can be repeated.
Sacral Neuromodulation (Interstim)
An electrode is placed adjacent to the sacral nerve roots (S3) through the sacral foramina, connected to a programmable implantable generator. Sacral neuromodulation modulates the afferent nerve signals from the bladder and pelvic floor — highly effective for interstitial cystitis / bladder pain syndrome, refractory bladder dysfunction, and pelvic floor hypertonicity contributing to CPP.
Cryoanalgesia — SurgiPartner’s Featured Technology
Cryoanalgesia applies precisely targeted cold energy (-70°C to -88°C) to a specific nerve — causing reversible wallerian degeneration (breakdown of the nerve’s myelin sheath and axon) without destroying the nerve’s supporting framework (endoneurium). The nerve transmits no pain signals for 3–12 months while regenerating along its preserved endoneurial tube. At SurgiPartner partner centres in Hyderabad, cryoanalgesia is applied to the superior hypogastric plexus, pudendal nerve, and iliohypogastric/ilioinguinal nerves for sustained pelvic pain relief with an excellent safety profile — no risk of deafferentation pain (a serious risk with chemical neurolysis). Call +91 9030053009 to discuss cryoanalgesia for pelvic pain.
Trigger Point Injections — Myofascial Pelvic Floor Pain
For patients with hypertonic pelvic floor muscles and identifiable myofascial trigger points, injections of local anaesthetic (with or without botulinum toxin A) directly into the trigger points release the spasm and break the pain-spasm-pain cycle. Combined with pelvic physiotherapy, trigger point injections provide significant and durable relief for myofascial CPP.
Botulinum Toxin A — Pelvic Floor and Bladder
Botulinum toxin A (BTX-A) injected into hypertonic pelvic floor muscles provides 3–6 months of muscle relaxation — significantly reducing pain from pelvic floor spasm, vaginismus, and pudendal neuralgia components. BTX-A into the detrusor muscle (bladder wall) via cystoscopy reduces bladder pain and urgency in interstitial cystitis resistant to oral treatments.
💡 SurgiPartner’s multidisciplinary pain approach: Chronic pelvic pain is best managed by a team — pain specialist (interventional procedures), gynaecologist (endometriosis, adenomyosis), urologist (IC/BPS, CPPS), pelvic physiotherapist (pelvic floor rehabilitation), and psychologist (central sensitisation, CBT). SurgiPartner coordinates all these specialists in Hyderabad. Call +91 9030053009.
Frequently Asked Questions — Pelvic & Abdominal Pain Treatment Hyderabad
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing expert care, advanced technology, and a commitment to restoring full mobility. Our approach to ACL Reconstruction Surgery helps athletes and active individuals regain knee stability, confidence, and performance.
01.
Experienced Sports Orthopedic Surgeons
Our skilled surgeons specialize in ACL reconstruction, ligament repair, and sports injury management, ensuring precision and faster return to activity.
02.
Advanced Arthroscopic & Minimally Invasive Techniques
We use keyhole surgical methods that reduce scarring, pain, and recovery time promoting faster joint healing
03.
Personalized Rehabilitation Programs
Each recovery plan is custom-designed with physiotherapists to restore flexibility, strength, and confidence step by step.
04.
Fast, Pain-Free Recovery
Most patients start walking within days and return to sports or active routines within a few months supported by guided rehab care.
Book Your Consultation
Take the first step toward stronger, more stable knees with SurgiPartner advanced ACL Reconstruction Surgery. Our specialists are here to guide you through a safe and effective recovery journey.
Get back in the game – that’s the SurgiPartner promise
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.