Relieve Pain. Prevent Recurrence. Regain Shoulder Confidence
Restore Shoulder Stability with SurgiPartner Advanced Shoulder Dislocation Management
Shoulder Dislocation Treatment in Hyderabad
Shoulder dislocation is the most common major joint dislocation treated in emergency departments — and without the right treatment, it becomes a recurring problem that progressively damages your shoulder’s stabilising structures. SurgiPartner connects patients across Hyderabad with specialist shoulder surgeons for comprehensive dislocation evaluation, acute reduction, and definitive surgical stabilisation. Whether it’s your first dislocation or a chronic instability problem, our expert team ensures you receive the most appropriate treatment to prevent recurrence and protect your long-term shoulder function.


What Is Shoulder Dislocation? Understanding the Anatomy
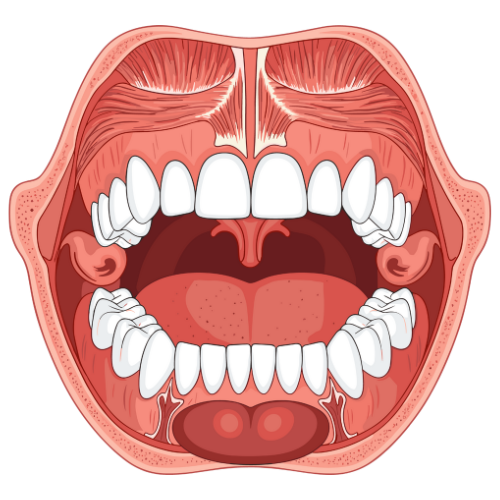
The shoulder (glenohumeral) joint is the most mobile joint in the human body — it can move in more directions than any other joint, allowing us to reach overhead, behind the back, and across the body. This extraordinary range of motion comes at a cost: the shoulder is inherently less stable than deeper ball-and-socket joints like the hip.
The glenohumeral joint works like a golf ball (the humeral head) sitting on a golf tee (the shallow glenoid socket of the scapula). Stability depends almost entirely on soft tissue structures: the glenoid labrum (a fibrocartilaginous rim that deepens the socket), the glenohumeral ligaments (capsular ligaments that constrain excessive movement), and the rotator cuff muscles (which dynamically stabilise the joint during movement).
A shoulder dislocation occurs when the humeral head is forced completely out of the glenoid socket. This is distinct from a subluxation, where the humeral head partially slips out but returns spontaneously. Both require specialist evaluation — subluxations frequently progress to full dislocations without proper treatment.
Types of Shoulder Dislocation — Anterior, Posterior and Inferior
Anterior Dislocation — 95% of All Cases
The humeral head is forced forward and downward out of the glenoid socket. The mechanism is typically forced abduction, extension, and external rotation of the arm — as occurs in a cricket bowling action, swimming freestyle stroke, martial arts throw, or a fall on an outstretched hand. The shoulder appears flattened at the front, with a prominent bump visible where the humeral head has displaced.
Typical injuries caused by anterior dislocation:
- Bankart lesion — tear of the anterior glenoid labrum from the glenoid rim. Present in over 90% of first-time anterior dislocations. This is the primary cause of recurrent instability.
- Hill–Sachs lesion — a compression fracture on the posterior superior humeral head caused by impact against the anterior glenoid rim during dislocation. Present in 40–90% of anterior dislocations.
- Bony Bankart lesion — when the anterior glenoid rim fractures, taking a fragment of bone with the labrum. Significantly increases recurrence risk and may require the Latarjet procedure.
- Axillary nerve injury — the axillary nerve runs close to the inferior joint capsule and is stretched or contused in 5–35% of anterior dislocations. Causes weakness of the deltoid muscle and numbness over the outer shoulder. Usually recovers within 3–6 months.
- Rotator cuff tear — more common in patients over 40 years; the subscapularis tendon is particularly vulnerable during anterior dislocation.
Posterior Dislocation — Less Than 5% of Cases
The humeral head is displaced posteriorly behind the glenoid. Classic causes include electric shock (involuntary muscle contraction), epileptic seizure, heavy fall directly onto the front of the shoulder, or bench press with excessive weight. Posterior dislocation is frequently missed on initial evaluation — the shoulder may appear almost normal and the patient can internally rotate the arm. The key X-ray sign is the “light bulb” appearance on AP view and the “trough sign” from posterior glenoid rim impaction (reverse Hill–Sachs lesion).
Inferior Dislocation (Luxatio Erecta)
Extremely rare. The arm is locked in hyperabduction with the humeral head displaced inferiorly and the arm pointing upward. Caused by violent hyperabduction forces. Associated with high rates of neurovascular and rotator cuff injury requiring urgent surgical attention.
Acute Management — What Happens at the Emergency Department
If you or someone near you has dislocated their shoulder, immobilise the arm in the most comfortable position (do not try to force it back yourself — this risks fracture and neurovascular injury) and go to the nearest emergency department or call SurgiPartner at +91 9030053009 for immediate guidance.
In the emergency setting, X-rays confirm the dislocation and exclude associated fractures. The shoulder is then reduced (put back in place) using one of several established techniques under intravenous pain medication and muscle relaxants or procedural sedation:
- Cunningham technique — gentle muscle massage and positioning without traction; lowest risk of complications
- Stimson technique — patient lies prone with the arm hanging, gentle weights applied to relax the muscles
- Milch technique — gentle abduction and external rotation to guide the humeral head back to the socket
- Kocher’s manoeuvre — older technique; effective but higher risk of iatrogenic fracture if applied forcefully
After successful reduction, the shoulder is confirmed in position with post-reduction X-rays. A sling is applied for comfort. The critical question that follows — whether surgical stabilisation is needed — is determined by factors including the patient’s age, activity level, labral injury extent, bone loss, and recurrence risk.


Who Is at Risk of Recurrent Shoulder Dislocation?
The recurrence risk after a first-time anterior shoulder dislocation is strongly predicted by age at first dislocation — the younger the patient, the higher the recurrence risk with conservative treatment alone:
| Age at First Dislocation | Recurrence Rate (Conservative Tx) | Recommendation |
|---|---|---|
| Under 20 years | 80–90% | Strong case for surgical stabilisation after first dislocation |
| 20–30 years | 60–80% | Surgical stabilisation recommended for active/athletic patients |
| 30–40 years | 40–60% | Discuss risks and benefits; surgical stabilisation for active patients |
| Over 40 years | 10–20% | Trial of conservative treatment; operate if recurrence or rotator cuff tear |
Additional risk factors for recurrence include: participation in contact or overhead sports (cricket, kabaddi, martial arts, swimming), male sex, significant bone loss from the glenoid or humeral head, a large Hill-Sachs lesion that engages over the glenoid rim during activity (off-track lesion), and failure to complete physiotherapy.
Shoulder Stabilisation Surgery — Bankart Repair vs Latarjet Procedure
Arthroscopic Bankart Repair
Bankart repair is the gold-standard surgical treatment for recurrent anterior shoulder instability without significant bone loss. The procedure is performed entirely arthroscopically through 3 small portals (approximately 5–7mm each).
The surgeon uses a suture anchor system to reattach the torn anterior labrum firmly back to the glenoid rim, recreating the labral bumper that prevents forward humeral head displacement. The anterior capsule is also tensioned (capsulorrhaphy) to restore normal capsular constraint. Modern suture anchor systems (knotless, biocomposite, or titanium) provide excellent fixation strength — sufficient to allow progressive rehabilitation while the repair heals biologically over 4–6 months.
When Bankart repair is the right choice:
- Recurrent anterior instability with intact or minimally eroded glenoid bone stock (less than 15–20% glenoid bone loss)
- Soft tissue Bankart lesion confirmed on MRI arthrogram
- On-track Hill–Sachs lesion (not engaging over the glenoid during movement)
- First dislocation in young high-risk athletes who wish to avoid prolonged physiotherapy
- Failed conservative management in appropriate patients
Success rate: 85–92% for prevention of recurrent dislocation in patients without bone loss. In patients with bone loss greater than 20%, recurrence rates increase — in these cases, the Latarjet procedure is preferred.
Latarjet Procedure (Coracoid Transfer)
The Latarjet procedure is a more complex but highly effective surgical solution for patients with significant glenoid bone loss, failed Bankart repair, or high-risk contact sport athletes. The coracoid process — a bony projection from the front of the scapula with its attached conjoint tendon — is detached and transferred to the anterior glenoid rim using two screws.
This transfer accomplishes three simultaneous objectives: it enlarges the glenoid articular surface (replacing lost bone), creates a sling effect from the conjoint tendon (dynamically blocking anterior humeral head displacement), and provides capsular reinforcement. This triple mechanism makes the Latarjet uniquely robust, with recurrence rates under 5% even in high-risk athletes.
When the Latarjet is preferred:
- Glenoid bone loss greater than 20% (confirmed on 3D CT scan)
- Off-track Hill–Sachs lesion engaging the glenoid rim during external rotation
- Failed Bankart repair
- High-risk contact or throwing sport athletes requiring maximum stability
- Epileptic patients at high risk of traumatic dislocation during seizure
The Latarjet is performed through a 5–6cm deltopectoral approach under general anaesthesia with an interscalene nerve block for post-operative pain control. Hospital stay: 1–2 nights. The screws and transferred coracoid are confirmed on post-operative X-ray.
Remplissage (Hill–Sachs Filling)
Combined with Bankart repair, the infraspinatus tendon and posterior capsule are arthroscopically sutured into the Hill–Sachs defect on the humeral head — physically filling it to prevent engagement against the anterior glenoid rim. Remplissage is indicated for moderate Hill–Sachs lesions in patients where a Latarjet would otherwise be needed due to on-track lesion concerns. It allows a less invasive solution for selected patients while preserving shoulder motion better than previously expected.
Shoulder Stabilisation Surgery — Bankart Repair vs Latarjet Procedure
| Procedure | Approach | Best For | Recurrence Rate | Return to Sport | Key Risk |
|---|---|---|---|---|---|
| Bankart Repair | Arthroscopic (3 portals) | No/minimal bone loss, soft tissue Bankart | 8–15% | 4–5 months | Higher recurrence with bone loss |
| Latarjet | Open deltopectoral (5–6cm) | Bone loss >20%, failed Bankart, contact athletes | <5% | 5–6 months | Hardware complications, neurovascular proximity |
| Remplissage + Bankart | Arthroscopic | Moderate Hill-Sachs, on-track lesion | 5–8% | 5–6 months | Mild external rotation loss |
Why Choose SurgiPartner for Shoulder Dislocation Treatment in Hyderabad?
| Phase | Timeline | Goals | Activities Permitted |
|---|---|---|---|
| Immobilisation | Weeks 0–4 (Bankart) / 0–3 (Latarjet) | Protect repair, control swelling | Gentle pendulum exercises, elbow and wrist ROM |
| Early Mobilisation | Weeks 4–8 | Restore full passive range of motion | Passive and active-assisted exercises, pool therapy |
| Strengthening | Months 2–4 | Rotator cuff and scapular stabiliser strength | Progressive resistance exercises, light gym work |
| Sport-Specific Training | Months 4–6 | Sport-specific movement patterns, agility | Throwing, overhead drills, non-contact sport participation |
| Return to Full Sport | Months 5–9 | Clearance testing and return to full contact/overhead sport | Full sport participation with surgeon clearance |
Why Choose SurgiPartner for Shoulder Dislocation Treatment in Hyderabad?
Modern shoulder replacement implants are designed to last 15–25+ years. Registry data shows over 90% of total shoulder replacements functioning well at 10 years and approximately 85% at 15 years. Reverse total shoulder replacements show similar or slightly better survival rates due to the inherent stability of the reversed construct. Implant longevity is influenced by patient activity level, body weight, implant design, and the precision of surgical component positioning. Glenoid component loosening (in anatomic TSA) has historically been the primary cause of long-term failure, which modern implant designs and surgical techniques have significantly reduced.
In a total shoulder replacement (TSA), the anatomy is recreated normally — the metal ball replaces the humeral head and a plastic socket replaces the glenoid. This requires an intact rotator cuff to function properly. In a reverse shoulder replacement (RTSA), the ball and socket are switched — a metal ball is attached to the glenoid, and a socket is attached to the humerus. This reversal allows the deltoid muscle to power shoulder elevation independently of the rotator cuff, making RTSA the only reliable solution for patients with combined arthritis and massive rotator cuff failure. The choice between TSA and RTSA is primarily determined by the status of the rotator cuff — assessed on MRI before surgery.
Shoulder replacement with a modern anaesthesia protocol — combining general anaesthesia and an interscalene nerve block — results in very well-controlled post-operative pain. The nerve block provides 12–18 hours of complete shoulder numbness post-operatively, during which most patients are very comfortable. The following 48–72 hours involve moderate aching effectively managed with prescribed oral analgesics. Patients consistently report that their pre-operative chronic arthritis pain is far worse than the surgical recovery pain. Most patients experience significant pain reduction within 4–6 weeks and are very satisfied with their overall pain levels by 3 months.
The main restriction after total or reverse shoulder replacement relates to subscapularis healing in the first 6 weeks: avoid forceful internal rotation (reaching behind the back), pushing yourself up from a chair with the operated arm, or lifting objects heavier than a cup of tea. These restrictions protect the subscapularis tendon repair while it heals. After 6 weeks, most restrictions are progressively lifted based on functional recovery. Long-term: most low-impact activities are unrestricted. High-impact activities involving risk of fall or contact (such as cricket, martial arts) are generally discouraged to protect implant longevity, though guidelines are becoming more liberal with modern implant designs. Your SurgiPartner surgeon will provide personalised guidance based on your specific implant and recovery.
Yes — shoulder replacement surgery for medical indications (osteoarthritis, rotator cuff arthropathy, rheumatoid arthritis, AVN, or fracture) is covered by all major health insurance plans in India including Star Health, HDFC Ergo, Niva Bupa, United India, New India Assurance, and Ayushman Bharat for eligible patients. The implant cost is typically the largest component. SurgiPartner's dedicated insurance coordination team verifies your specific policy benefits before surgery and manages the entire cashless claim process, including pre-authorisation and final billing. Call +91 9030053009 for a free insurance check.
Bilateral simultaneous shoulder replacement (both shoulders done in one anaesthetic episode) is very rarely performed due to the significant rehabilitation challenge — patients need at least one functional arm to assist recovery and daily activities. Staged bilateral replacement — one shoulder at a time, typically 3–6 months apart — allows full recovery of the first shoulder before operating on the second. Most patients with bilateral severe shoulder arthritis opt for the most symptomatic side first and decide on the second based on functional improvement and remaining symptom burden. SurgiPartner's team will discuss the most appropriate sequence based on your specific situation.
Driving is generally not permitted for 6–8 weeks after shoulder replacement surgery. The sling is worn for the first 4–6 weeks, during which driving is impossible. After sling removal, driving clearance requires: adequate range of motion to control the steering wheel and gear shift, sufficient strength for emergency braking and steering, no opioid pain medication affecting alertness, and surgical clearance from your SurgiPartner orthopaedic surgeon. Automatic transmission vehicles can typically be driven sooner than manual (stick shift) vehicles. Your specific clearance timing will depend on which shoulder was operated and your individual recovery progress
Pseudoparalysis is the inability to actively lift the arm above shoulder height despite having full passive range of motion (when someone else lifts your arm, it goes to full elevation). It is caused by massive rotator cuff tearing that removes the dynamic centring force on the glenohumeral joint, allowing the humeral head to migrate superiorly when the deltoid contracts. Pseudoparalysis is the hallmark of rotator cuff arthropathy — one of the primary indications for reverse total shoulder arthroplasty. RTSA's reversed geometry lowers and medialises the rotation centre, dramatically increasing the deltoid's mechanical advantage and allowing it to power full active elevation even without any rotator cuff function. Most patients with pseudoparalysis achieve active elevation above 120° after RTSA.
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing trusted orthopedic care with advanced shoulder expertise.
01.
Expert Shoulder & Sports Injury Surgeons
Our specialists have extensive experience managing acute and recurrent shoulder dislocations.
02.
Advanced Surgical Technology
We use modern minimally invasive techniques for precise ligament repair.
03.
Personalized Treatment Plans
Each patient receives a customized plan based on injury severity and activity level.
04.
Safe & Compassionate Care
Most patients regain shoulder confidence and mobility with reduced recurrence risk.
Book Your Consultation
Take the first step toward stable, pain-free shoulder movement with SurgiPartner advanced shoulder dislocation management. Our experts are here to guide you through safe, effective, and lasting care.
Stable shoulders. Confident movement.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.