Say Goodbye to Hernia Discomfort with SurgiPartner Advanced Hernia Treatments
Experience Safe, Scar-Free Recovery with Precision Laparoscopic Care
Hernia Treatment in Hyderabad — Laparoscopic Hernia Repair
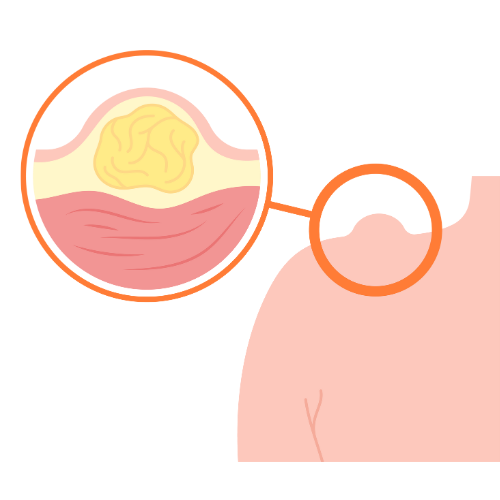
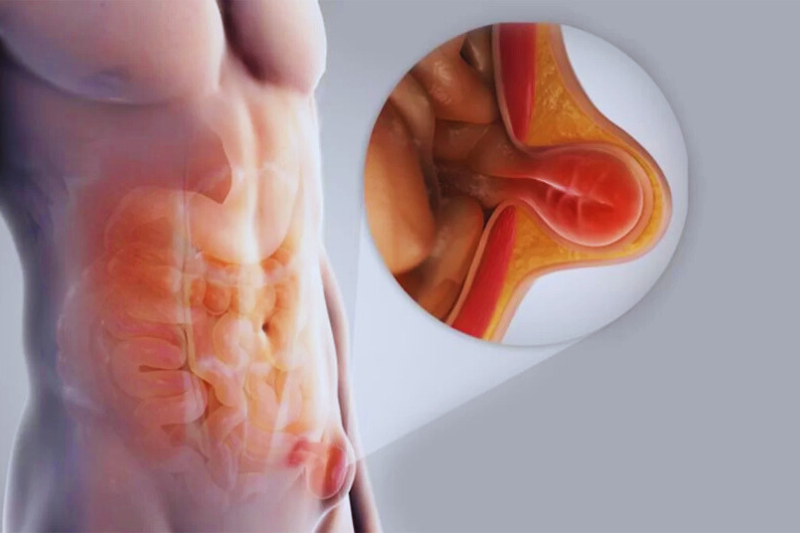
A hernia occurs when an internal organ or fatty tissue protrudes through a weakness or hole in the surrounding muscle or connective tissue wall. Hernias are one of the most common conditions requiring general surgical intervention — with over 20 million hernia repairs performed globally each year. In Hyderabad, SurgiPartner connects patients with experienced general surgeons for laparoscopic hernia repair — the minimally invasive technique that provides faster recovery, less pain, and lower recurrence rates compared to traditional open surgery.
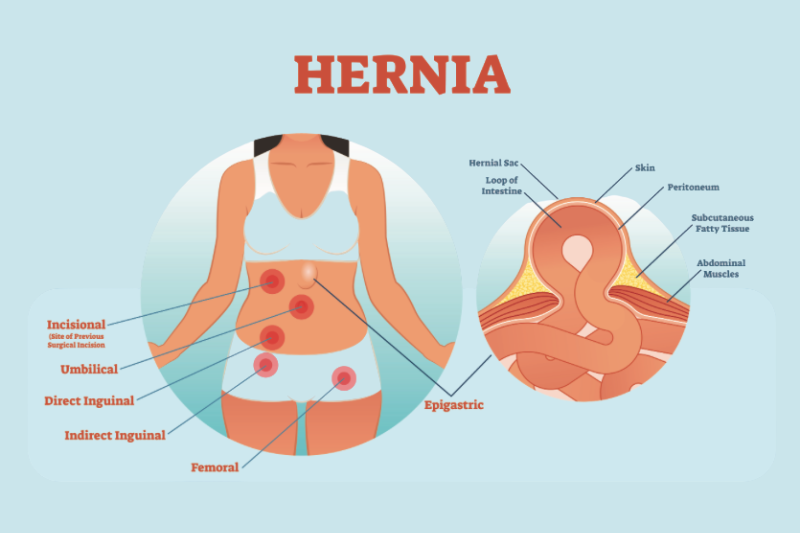
Types of Hernia — Complete Classification
Inguinal Hernia (Most Common — 75% of All Hernias)
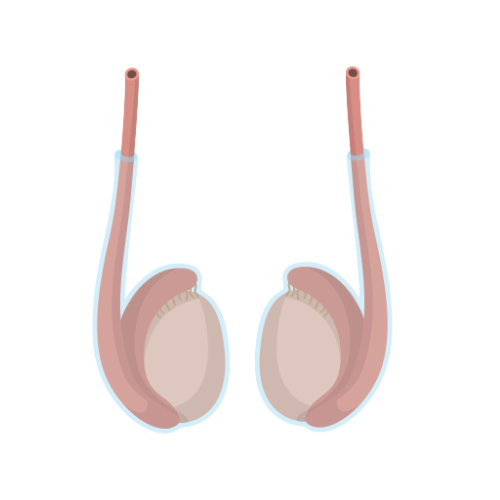
Inguinal hernias occur in the groin region when abdominal contents protrude through the inguinal canal — a passage in the lower abdominal wall through which the vas deferens passes in men (and the round ligament of the uterus in women). They are significantly more common in men (8:1 male:female ratio) due to the wider inguinal canal left by testicular descent during foetal development.
- Indirect inguinal hernia — the most common type; hernia sac passes through the internal inguinal ring along the path of the vas deferens; may extend into the scrotum (inguino-scrotal hernia) in men. Congenital component — patent processus vaginalis — is frequently present.
- Direct inguinal hernia — hernia protrudes directly through the weakened posterior wall of the inguinal canal (Hesselbach’s triangle) rather than through the ring; more common in older men; associated with chronic raised intra-abdominal pressure (chronic cough, constipation, heavy lifting, obesity).
Umbilical Hernia
Umbilical hernias protrude through the umbilical ring — most common in infants (typically closing spontaneously by age 3–4), and in adults particularly in women after pregnancy, obese individuals, and those with cirrhosis and ascites. Adult umbilical hernias do not close spontaneously and require surgical repair.
Incisional Hernia
Occurs through a previous surgical incision site where the abdominal wall has weakened. Risk factors include obesity, wound infection, poor nutrition, steroid use, and tension on the original closure. Incisional hernias are the most challenging to repair due to variable size, loss of domain, and requirement for larger mesh coverage.
Femoral Hernia
Protrudes through the femoral canal below the inguinal ligament. More common in women. Carries a high strangulation risk (up to 40% of cases present as emergencies) due to the narrow, rigid femoral ring — making early elective repair essential on diagnosis.
Hiatal Hernia
A portion of the stomach protrudes through the oesophageal hiatus (opening) in the diaphragm into the chest. Classified as: Type I (sliding) — gastro-oesophageal junction moves above the diaphragm (most common, associated with GORD); Type II–IV (paraesophageal) — fundus or complete stomach herniates beside the oesophagus (requires surgical repair due to strangulation risk). Treated with laparoscopic fundoplication (Nissen or Toupet).
Epigastric, Spigelian, and Lumbar Hernias
Less common hernias that require specialist assessment. Epigastric hernias protrude through the linea alba above the navel. Spigelian hernias occur along the lateral border of the rectus muscle and are particularly difficult to diagnose clinically (CT or ultrasound required). Lumbar hernias protrude through the lumbar triangle.

When Does a Hernia Need Surgery?
- Symptomatic hernia — pain, discomfort, dragging sensation, or restriction of daily activities warrant elective repair. The discomfort typically worsens with activity and relieves with lying down.
- Irreducible hernia — a hernia that cannot be pushed back into the abdomen (non-reducible) requires urgent surgical assessment; it may progress to incarceration or strangulation.
- Incarcerated hernia — the hernia contents are trapped and cannot be reduced; bowel may become obstructed — surgical emergency.
- Strangulated hernia — the blood supply to the incarcerated hernia contents is compromised; bowel necrosis occurs rapidly — life-threatening surgical emergency requiring immediate operation.
- Femoral hernia — high strangulation risk; all femoral hernias should be repaired promptly on diagnosis regardless of symptoms.
- Watchful waiting for asymptomatic inguinal hernia — current guidelines (EHS 2018) support watchful waiting for asymptomatic or minimally symptomatic inguinal hernias in low-risk patients, as the annual risk of strangulation is approximately 0.2%. However, most patients are advised repair to prevent symptom progression and avoid the higher surgical risk of emergency repair.
⚠️ Emergency signs of hernia strangulation: Sudden severe pain in the hernia site; the hernia becomes hard, tender, and irreducible; nausea and vomiting; fever; signs of bowel obstruction (abdominal distension, no bowel movement). This is a surgical emergency — call +91 9030053009 or go to the nearest emergency department immediately.
Laparoscopic Hernia Repair — TAPP vs TEP
TAPP — Transabdominal Preperitoneal Repair
In TAPP, the surgeon enters the peritoneal (abdominal) cavity and then creates a preperitoneal space behind the abdominal wall to place the mesh. Three ports are used (umbilical + two lateral). The peritoneal flap is opened to expose the inguinal floor; the hernia sac is dissected and reduced; a large mesh (10–15cm) is placed covering all potential hernia sites in the groin; the peritoneum is closed over the mesh to prevent bowel contact. TAPP provides excellent visualisation and allows simultaneous bilateral hernia repair in the same anaesthetic. Also allows diagnosis and treatment of other peritoneal conditions (e.g. unexpected contralateral hernia, peritoneal disease).
TEP — Totally Extraperitoneal Repair
TEP is performed entirely in the preperitoneal space without entering the peritoneal cavity. A balloon dissector creates the preperitoneal space; the three operating ports remain extraperitoneal throughout; mesh is placed without requiring peritoneal closure. TEP theoretically reduces the risk of intraperitoneal injury and adhesion formation. Technically more demanding than TAPP — the surgeon must navigate in a narrower extraperitoneal plane without the benefit of the peritoneal cavity as a working space.
| Feature | TAPP | TEP | Open (Lichtenstein) |
|---|---|---|---|
| Approach | Through peritoneal cavity to preperitoneal space | Entirely preperitoneal — no peritoneal entry | Open groin incision; anterior repair |
| Learning curve | Moderate | Steeper | Well established, straightforward |
| Bilateral repair | Excellent — same ports | Good — same ports | Two separate incisions required |
| Recurrence rate | <2% (long-term) | <2% (long-term) | ~3–5% (long-term) |
| Chronic groin pain | Lower than open | Lower than open | Higher (nerve entrapment risk) |
| Recovery | 1–2 weeks return to work | 1–2 weeks return to work | 3–4 weeks return to work |
| Best for | Bilateral hernias; recurrent hernias; complex anatomy | Experienced laparoscopic surgeons; smaller hernias | Previous laparoscopic failure; emergency repair |
Laparoscopic Hernia Repair — TAPP vs TEP
Mesh reinforcement is the international standard for hernia repair — significantly reducing recurrence rates compared to primary tissue repair (suture-only repair). Modern hernia mesh types used at SurgiPartner partner hospitals:
- Polypropylene mesh — the most widely used; lightweight variants (40–45g/m²) are preferred as they provoke less inflammatory reaction and have lower chronic pain rates than heavyweight mesh; permanent, incorporated into surrounding tissue
- Composite mesh — one side is non-adhesive (PTFE, oxidised cellulose, or collagen) for the peritoneal surface; the other side is polypropylene for tissue ingrowth. Used when mesh will be placed in contact with bowel (intraperitoneal repair)
- Biologic mesh — derived from human or animal tissue; used in infected fields where synthetic mesh cannot be placed; absorbs over time; expensive; reserved for complex contaminated cases
- Self-gripping mesh — has small hooks that anchor the mesh without sutures or tacks; reduces risk of tack-related nerve injury
Frequently Asked Questions — Hernia Treatment Hyderabad
Yes — hernia surgery is covered under all health insurance policies in India as a medically indicated surgical procedure. This includes inguinal, umbilical, incisional, femoral, and hiatal hernia repairs. Pre-authorisation requires clinical documentation of the hernia diagnosis, relevant symptoms, and surgical recommendation. Asymptomatic hernias may require additional justification. SurgiPartner handles the complete insurance pre-authorisation process, cashless admission, and claim processing at partner hospitals in Hyderabad. Most patients pay nothing out of pocket for elective hernia repair when they have active insurance coverage. Call +91 9030053009 to verify your coverage before booking.
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing expertise, technology, and compassionate care. Our approach to Hernia Treatment ensures minimal pain, faster healing, and lasting comfort with advanced laparoscopic techniques.
01.
Expert Ophthalmic Surgeons
Our highly skilled surgeons specialize in inguinal, umbilical, and ventral hernia repairs, performing procedures with exceptional precision and safety.
02.
Advanced Keyhole Surgery Technology
We use minimally invasive laparoscopic methods for reduced scarring, less pain, and quicker recovery compared to open surgery.
03.
Personalized Treatment Plans
Each hernia is unique - we evaluate every case individually to design the most effective and comfortable treatment approach.
04.
Pain-Free & Fast Recovery
Most patients are discharged the same day and return to normal activities within a few days with continuous post-surgery support and care.
Book Your Consultation
Take the first step toward a pain-free, active life with SurgiPartner Advanced Hernia Treatment. Our experts are here to provide precise, safe, and lasting relief.
Live free from pain and discomfort that’s the SurgiPartner promise.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.