Cancer Pain
Cancer Pain Treatment in Hyderabad — Interventional Pain Management
Cancer pain is one of the most feared and undertreated aspects of malignant disease — affecting approximately 55–65% of patients with active cancer treatment and 66–75% of patients with advanced or metastatic cancer. Adequate cancer pain control is not merely a matter of comfort — it is a fundamental human right recognised by the WHO, the International Association for the Study of Pain (IASP), and India’s National Cancer Control Programme. Despite available treatments, studies indicate that up to 40–50% of cancer patients in India receive inadequate pain control. SurgiPartner’s interventional pain management team in Hyderabad provides comprehensive cancer pain assessment and treatment — from WHO analgesic ladder optimisation to advanced interventional procedures including celiac plexus neurolysis, intrathecal drug delivery, and spinal cord stimulation — ensuring that every cancer patient deserves and receives excellent pain control.


Understanding Cancer Pain — Types, Mechanisms and Assessment
Cancer pain is one of the most feared and undertreated aspects of malignant disease — affecting approximately 55–65% of patients with active cancer treatment and 66–75% of patients with advanced or metastatic cancer. Adequate cancer pain control is not merely a matter of comfort — it is a fundamental human right recognised by the WHO, the International Association for the Study of Pain (IASP), and India’s National Cancer Control Programme. Despite available treatments, studies indicate that up to 40–50% of cancer patients in India receive inadequate pain control. SurgiPartner’s interventional pain management team in Hyderabad provides comprehensive cancer pain assessment and treatment — from WHO analgesic ladder optimisation to advanced interventional procedures including celiac plexus neurolysis, intrathecal drug delivery, and spinal cord stimulation — ensuring that every cancer patient deserves and receives excellent pain control.
Types of Cancer Pain by Mechanism
| Pain Type | Mechanism | Clinical Character | Treatment Implications |
|---|---|---|---|
| Nociceptive somatic pain | Direct tumour invasion or metastases in bone, muscle, or soft tissue; inflammatory mediators stimulating nociceptors | Well-localised; aching, gnawing, or throbbing; bone metastasis pain is constant with movement-related exacerbations | NSAIDs for bone pain (prostaglandin-mediated); opioids; bisphosphonates; radiotherapy to bone metastases |
| Nociceptive visceral pain | Tumour stretching, compressing, or infiltrating hollow viscera or organ capsule | Poorly localised; cramping, squeezing, or pressure-like; referred patterns (e.g. pancreatic cancer → back; liver capsule → right shoulder) | Opioids; celiac plexus block for upper abdominal visceral pain; hypogastric plexus block for pelvic visceral pain |
| Neuropathic pain | Tumour invasion or compression of peripheral nerves, nerve plexuses (brachial, lumbosacral), or spinal cord | Burning, shooting, electric shock-like, dysaesthesia; allodynia (pain from non-painful stimuli); often refractory to standard opioids | Adjuvant medications (gabapentinoids, TCAs, SNRIs); nerve blocks; spinal cord stimulation; targeted RT |
| Mixed pain | Combination of somatic, visceral, and neuropathic mechanisms | Multiple overlapping pain characters | Combination treatment targeting each mechanism |
| Breakthrough (incident) pain | Transient severe pain flares on a background of adequately controlled baseline pain; triggered by movement, coughing, or spontaneous | Rapid onset (<3 minutes), intense, brief (15–30 minutes) | Short-acting opioid (fentanyl buccal, oral morphine) for breakthrough; prevent by addressing trigger if possible |
The WHO Analgesic Ladder — The Foundation of Cancer Pain Management
The WHO three-step analgesic ladder remains the international standard for cancer pain pharmacological management — providing adequate pain control in approximately 70–80% of cancer patients when correctly applied:
- Step 1 (Mild pain — NRS 1–3): Non-opioid analgesics — paracetamol, NSAIDs (ibuprofen, diclofenac, celecoxib); adjuvant medications for neuropathic components (gabapentin, pregabalin, amitriptyline)
- Step 2 (Moderate pain — NRS 4–6): Weak opioids — tramadol, codeine (codeine is now less favoured due to variable metabolism); OR low doses of strong opioids. Continue non-opioids + adjuvants.
- Step 3 (Severe pain — NRS 7–10): Strong opioids — morphine (the gold standard reference opioid), oxycodone, hydromorphone, fentanyl patches, methadone; titrated to effective dose; continue non-opioids + adjuvants. There is NO ceiling dose for opioids in cancer pain — the correct dose is the one that controls the pain.
Key WHO ladder principles: By mouth (oral route preferred when feasible); By the clock (regular, scheduled dosing — not PRN); By the ladder (appropriate step for pain intensity); For the individual (dose individualisation); Attention to detail (anticipate and prevent side effects).

When the WHO Ladder Is Insufficient — Interventional Cancer Pain Management
Despite best pharmacological management, 20–30% of cancer pain patients have inadequate pain control due to: intolerable opioid side effects (severe nausea, constipation, sedation, confusion) limiting dose escalation; refractory neuropathic pain; specific anatomical pain patterns better targeted by interventional approaches; or patient preference to reduce opioid burden for quality of life reasons.
The WHO has extended the analgesic ladder to include a “Step 4” — interventional procedures — for patients who fail pharmacological management.
Celiac Plexus Neurolysis (CPN) — For Pancreatic and Upper Abdominal Cancer Pain
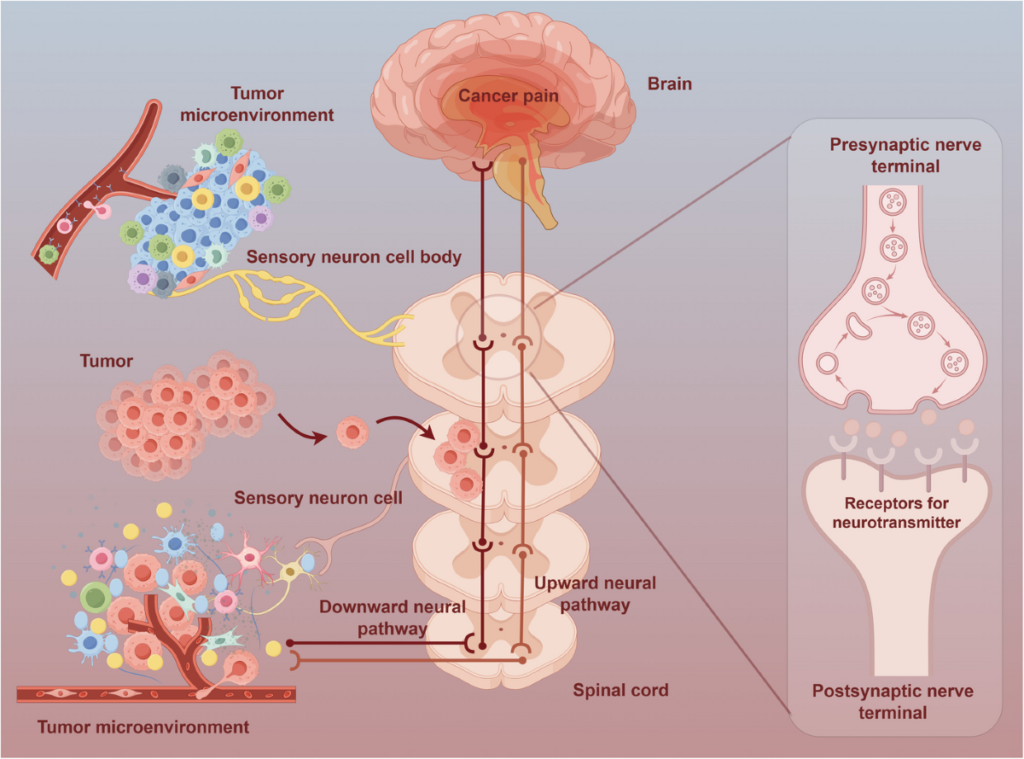
The celiac plexus is a network of sympathetic nerve fibres surrounding the aorta at the T12–L1 level, transmitting pain signals from all upper abdominal viscera — the stomach, pancreas, liver, gallbladder, small intestine, and upper colon. In pancreatic cancer — which causes some of the most refractory pain in oncology — celiac plexus neurolysis with absolute alcohol achieves 70–90% significant pain reduction in multiple randomised controlled trials, with reduced opioid requirements and improved quality of life. The effect typically lasts for the patient’s remaining disease duration (weeks to months).
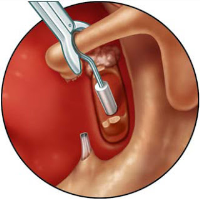
Technique: Performed under CT or fluoroscopic guidance, with the patient prone; bilateral needles are placed retroperitoneally at the T12–L1 level; absolute alcohol (50–100%) is injected after contrast confirmation of position. Alternatively, endoscopic ultrasound (EUS)-guided celiac plexus neurolysis accesses the plexus through the stomach wall under direct endoscopic vision — safer and increasingly preferred at specialist centres with EUS capability.
Superior Hypogastric Plexus Neurolysis — For Pelvic Cancer Pain
For cancer pain arising from pelvic malignancies — cervical cancer, endometrial cancer, rectal cancer, bladder cancer, prostate cancer — neurolysis of the superior hypogastric plexus with absolute alcohol achieves significant pain reduction in 70–85% of patients. As with celiac plexus neurolysis, this is an irreversible procedure using neurolytic agents rather than the reversible PRF or cryoanalgesia preferred for benign pain conditions — appropriate when the prognosis is limited and permanent nerve disruption is acceptable for the purpose of pain control.
Ganglion Impar Neurolysis — For Perineal Cancer Pain
For perineal, rectal, and anal cancer pain — particularly in patients with advanced anorectal malignancy where sitting, bowel movements, and any perianal activity cause severe pain — neurolysis of the ganglion impar provides very effective relief. Studies report 70–90% significant pain reduction in perineal cancer pain after ganglion impar neurolysis.
Intrathecal Drug Delivery (ITDD) / Spinal Drug Delivery System
An intrathecal catheter is placed in the cerebrospinal fluid (CSF) space of the spinal canal, connected to an implanted or external programmable pump that delivers precisely controlled doses of morphine (or other analgesic combinations — ziconotide, bupivacaine, clonidine) directly to the spinal cord — requiring only 1/300th of the systemic opioid dose for equivalent analgesia.
Indications for ITDD in cancer pain: inadequate pain control despite high-dose systemic opioids; intolerable systemic opioid side effects; neuropathic pain refractory to conventional treatment; patients with reasonable performance status (PS 0–2) and life expectancy of at least 3 months. The PACC (Poly Analgesic Consensus Conference) guidelines support ITDD as providing superior pain control with reduced side effects compared to systemic opioids for refractory cancer pain. Studies report 50–80% reduction in systemic opioid requirements after ITDD implantation.
Vertebroplasty / Kyphoplasty — For Painful Spinal Metastases
Painful vertebral body metastases causing pathological compression fractures and spinal instability are treated by percutaneous vertebroplasty (injection of bone cement into the fractured vertebral body) or balloon kyphoplasty (balloon inflation to restore vertebral height before cement filling). Both procedures provide rapid, effective pain relief for vertebral metastatic pain — with 70–85% significant pain reduction reported in multiple studies. Kyphoplasty provides the additional benefit of partial vertebral height restoration, reducing kyphotic deformity.
Radiotherapy — An Underutilised Analgesic
Palliative radiotherapy is one of the most effective treatments for localised bone pain from metastases — achieving 50–80% pain response rates. A single fraction (8 Gy) is as effective as multi-fraction courses (30 Gy in 10 fractions) for pain control in uncomplicated bone metastases and has a more convenient schedule for patients with limited performance status. EBRT (external beam RT) and SBRT (stereotactic body radiotherapy) are both effective. SurgiPartner’s pain team coordinates with oncology and radiotherapy services to ensure patients who may benefit from RT for pain are appropriately referred.
Epidural Steroid Injections and Nerve Root Blocks — For Radicular Cancer Pain
Cancer-related nerve root compression — from vertebral metastases, leptomeningeal disease, or tumour infiltration of the neural foramina — causes severe radicular pain (sciatica pattern, brachial plexus pain). Epidural steroid injections and selective nerve root blocks under fluoroscopic guidance provide targeted anti-inflammatory treatment — rapidly reducing radicular pain while systemic treatments (corticosteroids, chemotherapy, RT) begin to act.
💡 SurgiPartner’s cancer pain philosophy: “No cancer patient should suffer from pain that is treatable.” Our interventional pain team works alongside oncologists, palliative care physicians, and radiotherapists to ensure every patient with cancer pain has access to the full spectrum of modern pain management techniques.
Frequently Asked Questions — Cancer Pain Treatment Hyderabad
Chemotherapy-induced peripheral neuropathy (CIPN) is nerve damage caused by certain chemotherapy agents — platinum compounds (cisplatin, oxaliplatin), taxanes (paclitaxel, docetaxel), vinca alkaloids (vincristine), and bortezomib — causing numbness, tingling, burning, and pain in the hands and feet (glove-and-stocking distribution). It affects up to 30–40% of patients receiving these agents. Treatment: duloxetine is the only medication with Level A evidence for CIPN pain (significant reduction in pain scores in ASCO-endorsed RCTs); gabapentin and pregabalin are widely used with moderate evidence; topical amitriptyline/ketamine cream for peripheral application; scrambler therapy (non-invasive nerve stimulation); TENS; and dose modification or substitution of the causative agent when feasible. Smoking cessation, tight blood glucose control (in diabetics), and supplemental alpha-lipoic acid have some supportive evidence for prevention and management. SurgiPartner's pain specialists treat CIPN alongside the oncology team — call +91 9030053009.
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing expert care, advanced technology, and a commitment to restoring full mobility. Our approach to ACL Reconstruction Surgery helps athletes and active individuals regain knee stability, confidence, and performance.
01.
Experienced Sports Orthopedic Surgeons
Our skilled surgeons specialize in ACL reconstruction, ligament repair, and sports injury management, ensuring precision and faster return to activity.
02.
Advanced Arthroscopic & Minimally Invasive Techniques
We use keyhole surgical methods that reduce scarring, pain, and recovery time promoting faster joint healing
03.
Personalized Rehabilitation Programs
Each recovery plan is custom-designed with physiotherapists to restore flexibility, strength, and confidence step by step.
04.
Fast, Pain-Free Recovery
Most patients start walking within days and return to sports or active routines within a few months supported by guided rehab care.
Book Your Consultation
Take the first step toward stronger, more stable knees with SurgiPartner advanced ACL Reconstruction Surgery. Our specialists are here to guide you through a safe and effective recovery journey.
Get back in the game – that’s the SurgiPartner promise
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.