Get Quick Relief from Abdominal Pain with SurgiPartner Advanced Appendectomy
Prompt Diagnosis. Safe Surgery. Faster Recovery
Appendectomy Surgery in Hyderabad — Laparoscopic Appendix Removal
Appendicitis — inflammation of the appendix — is one of the most common acute surgical emergencies worldwide, affecting approximately 7–8% of the global population at some point in their lifetime. In Hyderabad, SurgiPartner connects patients with experienced general surgeons for emergency and elective appendectomy, including laparoscopic appendectomy — the minimally invasive gold standard that allows same-day discharge in many cases and full recovery within 1–2 weeks.


Understanding the Appendix — Anatomy and Function
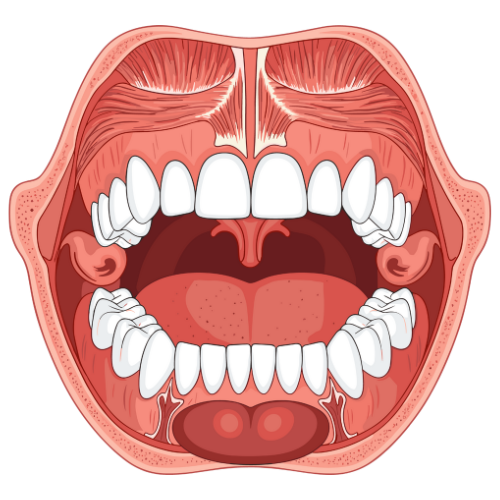
The appendix is a small, finger-shaped pouch approximately 5–10cm long that extends from the caecum (the beginning of the large intestine) in the right lower abdomen. Once considered a vestigial organ with no function, current evidence suggests the appendix serves as a reservoir for beneficial gut bacteria and plays a minor role in immune function — particularly in infancy. However, its absence after appendectomy has no clinically significant long-term consequences in adults.
Appendicitis occurs when the appendix becomes blocked — most commonly by hardened faecal material (faecolith), mucus, or lymphoid tissue hypertrophy following infection. The blocked appendix rapidly becomes infected by gut bacteria, inflamed, and swollen. Without treatment within 24–72 hours, the appendix can perforate (rupture) — releasing infected contents into the abdominal cavity and causing a life-threatening peritonitis. This is why appendicitis is treated as a surgical emergency.
Types of Appendicitis — Clinical Spectrum
| Type | Clinical Features | Management | Surgical Urgency |
|---|---|---|---|
| Uncomplicated acute appendicitis | Classic presentation; Alvarado score ≥7; no evidence of perforation on CT | Emergency laparoscopic appendectomy within 24 hours; antibiotics pre-operatively | Urgent — within 6–12 hours of diagnosis |
| Perforated appendicitis | Free air on imaging; peritonism on examination; high fever; elevated WBC and CRP | Emergency appendectomy; peritoneal lavage; IV antibiotics; drainage if abscess present | Emergency — immediate theatre |
| Appendiceal abscess / phlegmon | Palpable right iliac fossa mass; contained inflammation; days of symptoms | Interval appendectomy approach — IV antibiotics ± radiological drainage; elective appendectomy at 6–8 weeks | Urgent medical management; elective surgery later |
| Recurrent / chronic appendicitis | Multiple episodes of right iliac fossa pain without full resolution; milder symptoms | Elective laparoscopic appendectomy after workup to exclude other causes | Semi-elective — within weeks |


Diagnosis — Investigations Required
Clinical scoring — the Alvarado Score remains the bedrock of appendicitis diagnosis: points are allocated for migration of pain (1), anorexia (1), nausea/vomiting (1), right iliac fossa tenderness (2), rebound tenderness (1), elevated temperature (1), elevated white cell count (2), and left shift of differential (1). Score ≥7 indicates likely appendicitis; score ≥9 has >95% positive predictive value.
- Full blood count (FBC) — elevated WBC (typically 11,000–18,000 cells/μL); neutrophilia. Normal WBC does not exclude appendicitis — 20% of confirmed cases have a normal count initially.
- C-reactive protein (CRP) — elevated, often >40mg/L in established appendicitis; markedly elevated (>150mg/L) in perforated appendicitis
- Urine dipstick and pregnancy test — to exclude urinary tract infection and ectopic pregnancy (both cause right lower abdominal pain in women)
- Ultrasound abdomen and pelvis — first-line imaging in children, pregnant women, and younger women (to exclude ovarian pathology); operator-dependent; sensitivity for appendicitis approximately 75–85%
- CT scan abdomen with contrast — gold standard for adult appendicitis diagnosis; sensitivity >95%; identifies appendiceal wall thickening, periappendiceal fat stranding, appendicolith, free fluid, and perforation. Recommended when clinical diagnosis is uncertain or in atypical presentations.
- MRI — preferred alternative to CT in pregnant patients when ultrasound is inconclusive; no ionising radiation; sensitivity comparable to CT for appendicitis
Diagnosis — Investigations Required
Clinical scoring — the Alvarado Score remains the bedrock of appendicitis diagnosis: points are allocated for migration of pain (1), anorexia (1), nausea/vomiting (1), right iliac fossa tenderness (2), rebound tenderness (1), elevated temperature (1), elevated white cell count (2), and left shift of differential (1). Score ≥7 indicates likely appendicitis; score ≥9 has >95% positive predictive value.
- Full blood count (FBC) — elevated WBC (typically 11,000–18,000 cells/μL); neutrophilia. Normal WBC does not exclude appendicitis — 20% of confirmed cases have a normal count initially.
- C-reactive protein (CRP) — elevated, often >40mg/L in established appendicitis; markedly elevated (>150mg/L) in perforated appendicitis
- Urine dipstick and pregnancy test — to exclude urinary tract infection and ectopic pregnancy (both cause right lower abdominal pain in women)
- Ultrasound abdomen and pelvis — first-line imaging in children, pregnant women, and younger women (to exclude ovarian pathology); operator-dependent; sensitivity for appendicitis approximately 75–85%
- CT scan abdomen with contrast — gold standard for adult appendicitis diagnosis; sensitivity >95%; identifies appendiceal wall thickening, periappendiceal fat stranding, appendicolith, free fluid, and perforation. Recommended when clinical diagnosis is uncertain or in atypical presentations.
- MRI — preferred alternative to CT in pregnant patients when ultrasound is inconclusive; no ionising radiation; sensitivity comparable to CT for appendicitis
Laparoscopic Appendectomy — The Definitive Treatment
Laparoscopic appendectomy has replaced open appendectomy as the standard surgical approach for acute appendicitis at SurgiPartner partner hospitals in Hyderabad. The procedure is performed under general anaesthesia through three small keyhole incisions (5–12mm) in the abdomen.
Step-by-Step Procedure
- Port placement — a 10–12mm umbilical port (for the camera and specimen retrieval), and two 5mm working ports in the right lower abdomen and suprapubic area
- Pneumoperitoneum — the abdomen is insufflated with carbon dioxide gas to create working space; intra-abdominal pressure maintained at 12–15 mmHg
- Identification and mobilisation — the caecum is identified; the appendix is grasped at its tip and the mesoappendix (containing the appendiceal artery) is divided using a harmonic scalpel or haemoclips with electrosurgical division
- Ligation and division — the base of the appendix is doubly ligated with endoloops or stapled across with a linear endoscopic stapler; the appendix is divided
- Specimen retrieval — the appendix is placed in an endobag and retrieved through the umbilical port; sent for histopathological examination
- Lavage and closure — the abdominal cavity is irrigated with warm saline; ports are removed; fascial closure of the 12mm port; skin closed with absorbable sutures or clips
Procedure duration: 30–60 minutes for uncomplicated appendicitis; up to 90–120 minutes for perforated or complicated cases. Most uncomplicated appendectomy patients are discharged within 24 hours.
Advantages of Laparoscopic over Open Appendectomy
| Parameter | Laparoscopic | Open |
|---|---|---|
| Incision | Three small ports (5–12mm) | Single 5–8cm right iliac fossa incision (Lanz or Gridiron) |
| Post-op pain | Significantly less | More; wound site pain |
| Hospital stay | 24–48 hours (often same day) | 2–4 days |
| Return to work | 5–7 days (desk); 2 weeks (manual) | 2–4 weeks |
| Wound infection rate | ~2–3% | ~5–8% |
| Diagnostic advantage | Complete abdominal survey possible | Limited to right iliac fossa |
| Adhesion formation | Lower | Higher; future bowel obstruction risk |
Post-operative Recovery — Complete Timeline
- ours 1–6 post-op: Recovery from anaesthesia; pain well controlled with IV analgesia; IV fluids; clear liquids when alert and nausea-free
- Day 1: Light diet; mobilising; oral analgesia; most uncomplicated patients discharged with written instructions
- Days 2–5: Mild abdominal soreness; normal daily activities; avoid driving for 5–7 days; no heavy lifting (>5kg)
- Week 1–2: Return to desk work; port sites healing; absorbable sutures dissolving; full activity including light exercise
- Week 3–4: Return to manual work, gym, and all physical activity; no restrictions. Histopathology result reviewed at follow-up.
💡 SurgiPartner advantage: Our Care Buddy accompanies you from admission through recovery. Insurance pre-authorisation for appendectomy (a medically necessary emergency surgery) is handled by our team — covered under all health insurance plans. Call +91 9030053009 24 hours a day.
Frequently Asked Questions — Appendectomy Hyderabad
The warning signs of appendicitis that require immediate medical attention are: pain that begins around the navel and migrates to the right lower abdomen within a few hours; nausea and vomiting that follow the pain onset; loss of appetite; low-grade fever (37.5–38.5°C); and pain that worsens with movement or deep breathing. The critical distinguishing feature is the migration of pain from the navel to the right lower abdomen — this pattern is highly specific for appendicitis. Any right lower abdominal pain that has been worsening for more than 6 hours, or is accompanied by a temperature above 39°C or a rigid abdomen, is a surgical emergency requiring immediate hospital attendance. Call SurgiPartner on +91 9030053009 for 24-hour emergency surgical consultation in Hyderabad.
Recent research (particularly the APPAC and CODA trials) has shown that uncomplicated acute appendicitis — without perforation, abscess, or appendicolith on CT — can be successfully treated with antibiotics alone in approximately 70% of patients in the short term. However, of these patients, approximately 38% experience appendicitis recurrence within 5 years requiring eventual surgery. Non-operative management is particularly considered for patients at high anaesthetic risk or those who explicitly refuse surgery. At SurgiPartner Hyderabad, the standard treatment for appendicitis is laparoscopic appendectomy, which provides definitive, permanent cure. Antibiotic-only management is an individualised decision made with the patient after detailed counselling of the recurrence risk. Call +91 9030053009 for assessment.
Why Choose SurgiPartner?
Choosing SurgiPartner means choosing advanced surgical expertise with compassionate, patient-focused care.
01.
Expert Ophthalmic Surgeons
Our surgeons have extensive experience handling both emergency and planned appendectomy surgeries with precision and safety.
02.
Advanced Minimally Invasive Techniques
We use laparoscopic methods that reduce pain, scarring, hospital stay, and recovery time.
03.
Personalized Treatment Plans
Each patient receives a customized surgical and recovery plan based on infection severity and overall health.
04.
Pain-Free & Fast Recovery
Structured recovery support and follow-ups ensure smooth healing and long-term well-being.
Book Your Consultation
Take the first step toward relief from abdominal pain with SurgiPartner Advanced Appendectomy Surgery.
Live free from pain and discomfort that’s the SurgiPartner promise.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.