Minimally Invasive Ear Care • Faster Pain Relief • Improved Hearing
Quick Relief from Ear Pressure & Infection with SurgiPartner Myringotomy
Myringotomy in Hyderabad — Ear Tube Surgery, Grommets & Glue Ear Treatment
Myringotomy — a small controlled incision in the eardrum (tympanic membrane) to drain middle ear fluid and relieve pressure — is one of the most commonly performed procedures in paediatric ENT surgery worldwide. Combined with grommet (ventilation tube) insertion, myringotomy provides immediate middle ear ventilation, restores hearing, and dramatically reduces the frequency of ear infections in children affected by glue ear (otitis media with effusion) and recurrent acute otitis media. SurgiPartner connects families in Hyderabad with experienced paediatric ENT surgeons for myringotomy and ventilation tube insertion.


Understanding Glue Ear (Otitis Media with Effusion)
Glue ear is the accumulation of thick, sticky fluid in the middle ear space without signs of acute infection. It is the most common cause of acquired hearing loss in children — affecting up to 80% of children at some point before school age, with persistent bilateral glue ear affecting approximately 5% of school-age children at any given time. The fluid impairs eardrum mobility and ossicular vibration, causing conductive hearing loss of typically 25–40 dB — equivalent to hearing through ear muffs or from a considerable distance. In young children, this hearing loss during critical language development periods can delay speech acquisition and affect learning readiness.
Why Does Glue Ear Occur? — Eustachian Tube Dysfunction
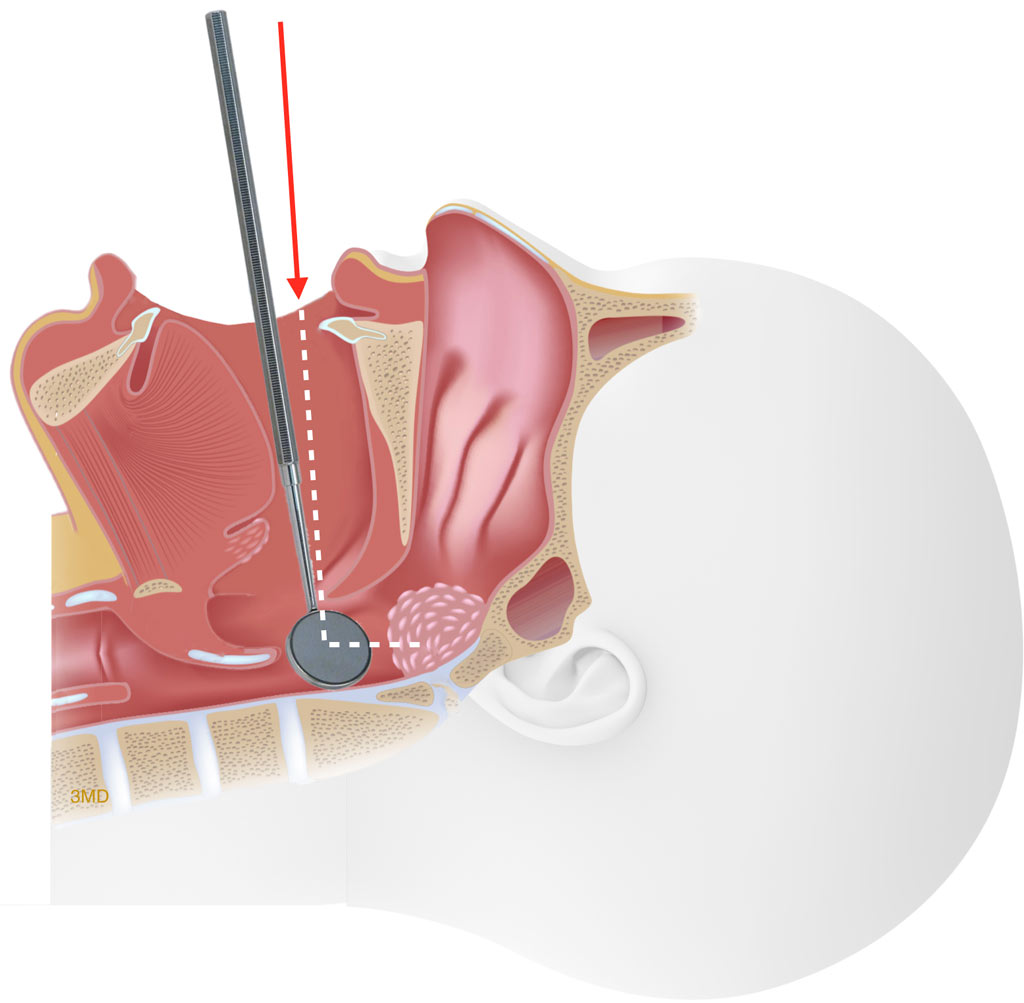
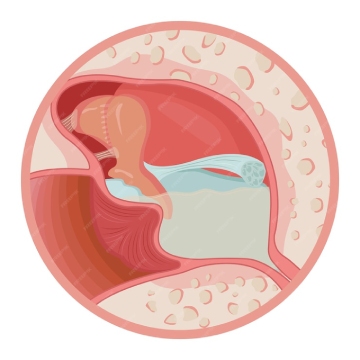
The Eustachian tube connects the middle ear to the nasopharynx (the back of the nose) and performs three critical functions: equalising middle ear pressure with atmospheric pressure, draining middle ear secretions, and protecting the middle ear from nasopharyngeal secretions. In children, the Eustachian tube is shorter, more horizontal, and more compliant than in adults — it functions less efficiently. When the Eustachian tube fails to open adequately (from adenoid hypertrophy, allergy, or repeated upper respiratory infections), the middle ear develops negative pressure, draws in fluid from the mucosa, and glue ear results.


When Is Myringotomy Recommended?
NICE (UK) and AAO-HNS (USA) guidelines recommend myringotomy with ventilation tube insertion when:
- Bilateral glue ear with hearing loss ≥25 dB HL has persisted for 3 months or longer
- Persistent glue ear is causing speech delay, learning difficulties, or behavioural problems attributable to hearing loss
- The child has had 3 or more acute ear infections in 6 months or 4 in 12 months, significantly disrupting family and school life
- Glue ear is associated with significant structural eardrum changes (atelectasis, early retraction pockets) indicating persistent negative middle ear pressure
- Adults have persistent middle ear effusion from Eustachian tube dysfunction following nasal surgery, radiotherapy, or barotrauma
Types of Ventilation Tubes (Grommets)
| Type | Design | Duration In Situ | When Used |
|---|---|---|---|
| Short-term (Shah / Shepard) | Small flanged bobbin; most commonly used | 6–12 months — extrude spontaneously | First-time insertion for glue ear or recurrent AOM |
| Long-term (T-tube / Goode) | T-shaped flange — resists spontaneous extrusion | 2–4 years — require surgical removal | Recurrent glue ear after multiple short-term tube insertions; Eustachian tube dysfunction expected to persist long-term |
| Titanium tubes | Metallic, corrosion-resistant | Variable — 12–18 months | Patients with MRI requirements or when biocompatibility is priority |
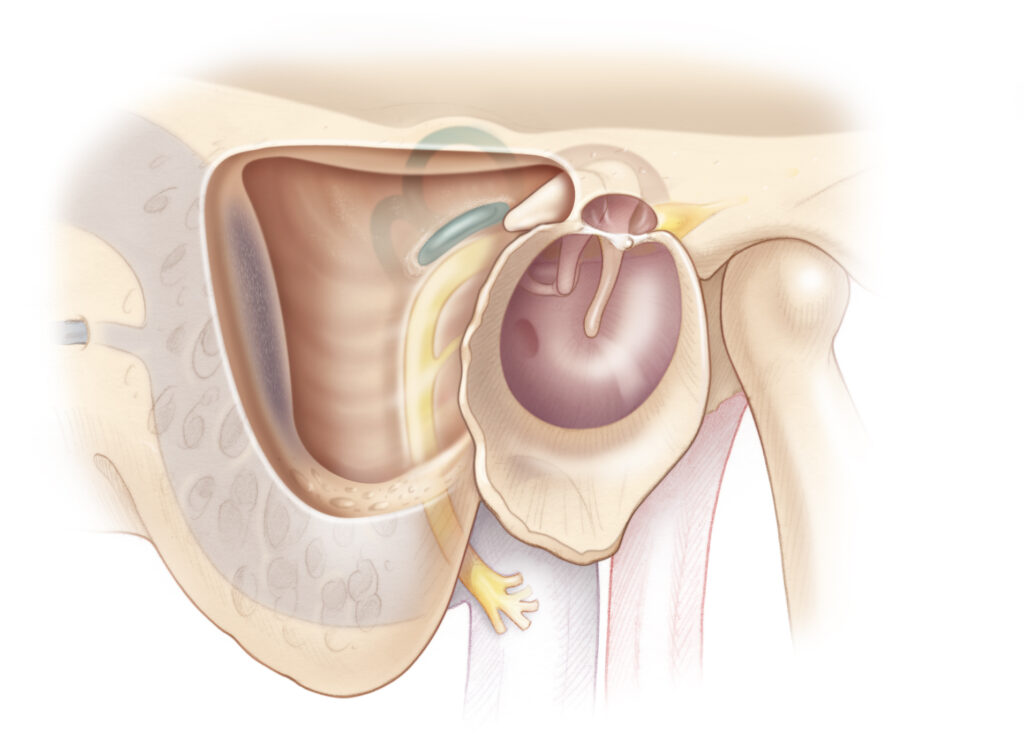
The Myringotomy Procedure — What Happens
In children, myringotomy is performed under brief general anaesthesia (mask induction, no intubation required for a procedure lasting only 10–15 minutes). In adults and older cooperative teenagers, myringotomy can be performed under local anaesthesia in the ENT clinic using an iontophoresis anaesthetic patch applied to the eardrum.
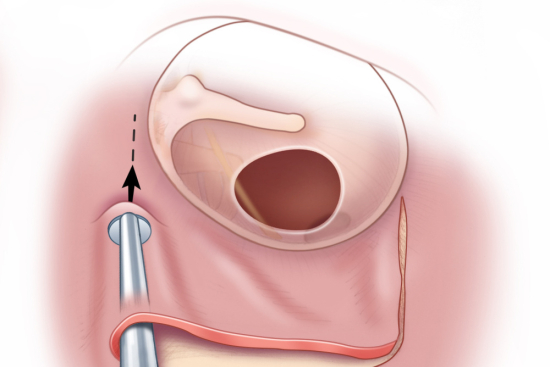
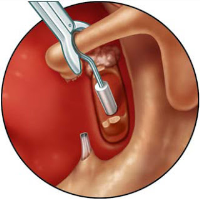
Under the operating microscope, a small radial or curvilinear incision is made in the antero-inferior or postero-inferior quadrant of the eardrum. Any middle ear fluid is aspirated — the thick glue-like consistency of chronic effusion confirms the clinical diagnosis. A ventilation tube (grommet) of the selected type is then inserted into the myringotomy incision — it clicks into position, held by the elasticity of the eardrum.
The entire procedure takes 5–15 minutes per ear. Children recover from the brief anaesthetic rapidly — most are eating and playing within 1–2 hours. Same-day discharge is the standard. Hearing improvement is immediate — many children (and their parents) comment on the dramatic change within hours of surgery.
Frequently Asked Questions — Myringotomy Hyderabad
Water precautions with grommets have been significantly revised based on evidence. Surface swimming — bath, pool, sea surface — is generally permitted without ear protection for standard grommets, as water pressure at the surface is insufficient to push water through the tube into the middle ear. Diving, jumping into water, and submersion are restricted — custom-moulded silicone ear plugs are recommended for these activities. Shampooing and showering without plugs are safe. Specific advice from your ENT surgeon regarding the grommet type inserted should always be followed. SurgiPartner provides written post-operative care instructions with all procedures.
When grommets extrude naturally, the small myringotomy incision heals promptly — typically within days to weeks — with no residual perforation in the vast majority of cases. Whether glue ear and ear infections recur depends on whether the underlying Eustachian tube dysfunction has resolved. In most children, Eustachian tube maturation occurs by age 7–8 — at which point the middle ear self-ventilates adequately and glue ear does not recur after grommet extrusion. In a minority with persistent Eustachian tube dysfunction, glue ear recurs and repeat grommet insertion (typically long-term T-tubes on the second insertion) may be required.
Why Choose SurgiPartner for Myringotomy?
Choosing SurgiPartner means choosing expert ENT care with advanced technology and compassionate support.
01.
Experienced ENT Specialists
Highly trained surgeons with extensive pediatric and adult ENT experience.
02.
Advanced Microscopic Techniques
Precise, minimally invasive procedures ensuring safety and comfort.
03.
Personalized Ear Care
Treatment tailored to age, infection severity, and hearing status.
04.
Complete Post-Procedure Support
Regular follow-ups, hearing assessments, and recovery guidance.
Book Your Consultation
Take the first step toward relief from abdominal pain with SurgiPartner Advanced Appendectomy Surgery.
Live free from pain and discomfort that’s the SurgiPartner promise.
Myringotomy – Patient Experiences
“My child’s ear infections stopped after myringotomy. Huge relief.”
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.