Regain Dignity & Comfort with SurgiPartner Advanced Genitourinary Fistula Repair
Expert Surgical Care • Minimally Invasive Techniques • Long-Term Relief
Genitourinary Fistula Repair in Hyderabad — VVF, Ureterovaginal & Urethrovaginal Fistula Surgery
A genitourinary fistula is an abnormal connection (tract) between the urinary tract and the reproductive organs — causing continuous, uncontrollable urinary leakage that profoundly affects quality of life. SurgiPartner Hyderabad connects patients with specialist urologists and gynaecological surgeons experienced in all types of genitourinary fistula repair, restoring urinary continence and dignity


Types of Genitourinary Fistula
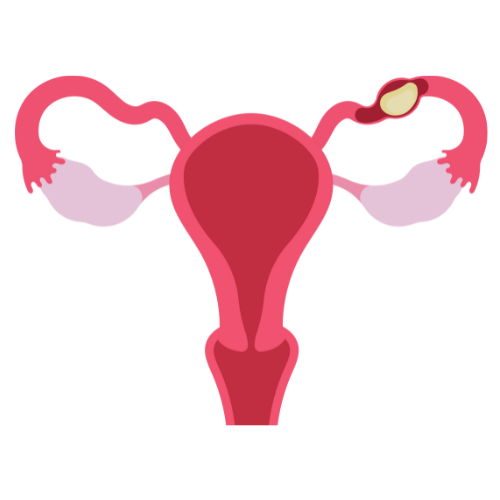
1. Vesicovaginal Fistula (VVF) — Most Common
A vesicovaginal fistula (VVF) is an abnormal opening between the bladder and the vagina. Urine leaks continuously from the bladder through this opening into the vagina, causing constant wetness, skin breakdown, recurrent infections, and severe social and psychological distress. VVF is the most common type of genitourinary fistula in developing countries, where obstetric complications are a leading cause.
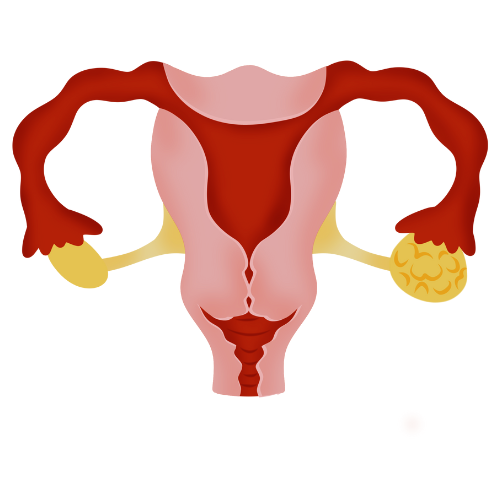
2. Ureterovaginal Fistula (UVF)
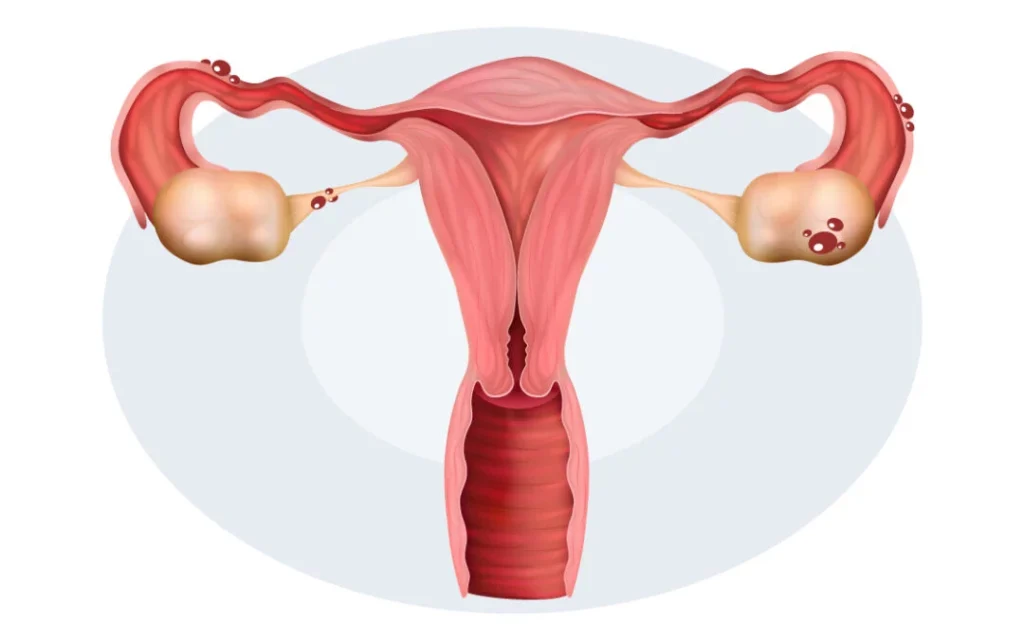
An abnormal connection between the ureter and the vagina, typically resulting from inadvertent ureteric injury during pelvic surgery. Patients experience constant leakage of urine from the vagina despite normal voiding, because the injured kidney continues to produce urine that drains directly through the fistula rather than through the bladder.
3. Urethrovaginal Fistula
An opening between the urethra and the vagina, causing urine leakage particularly during voiding. This type commonly results from difficult vaginal deliveries, anterior vaginal wall repairs, or urethral surgery. Patients experience urinary incontinence, spraying of urine, and sometimes vaginal voiding.
4. Vesicoenteric Fistula
An abnormal connection between the bladder and the bowel (usually sigmoid colon). Patients experience pneumaturia (air in the urine), faecaluria (faeces in the urine), recurrent urinary tract infections, and sometimes faecal material in the vagina. This type most commonly results from Crohn’s disease, diverticular disease, colorectal carcinoma, or pelvic radiation.
Causes of Genitourinary Fistula
| Cause | Mechanism | Fistula Type Most Common |
|---|---|---|
| Obstetric Injury | Prolonged obstructed labour causing pressure necrosis; instrumental delivery injury | VVF, Urethrovaginal |
| Surgical Injury | Hysterectomy, anterior colporrhaphy, pelvic floor repair, caesarean section | VVF, UVF, Urethrovaginal |
| Pelvic Radiation | Radiation-induced tissue damage and ischaemia after cervical/uterine/rectal cancer treatment | VVF, Vesicoenteric |
| Pelvic Malignancy | Cervical, bladder, or rectal cancer eroding tissue boundaries | VVF, Vesicoenteric |
| Inflammatory Bowel Disease | Crohn's disease causing transmural inflammation and fistulation | Vesicoenteric |
| Trauma | Pelvic fracture, penetrating injury | VVF, Urethrovaginal |
Diagnosis of Genitourinary Fistula
Accurate localisation and characterisation of the fistula are essential for surgical planning:
- 1. Clinical examination — pooling of urine in the vagina, identification of fistula opening on speculum examination
- 2. Three-swab test — dye (methylene blue) instilled into the bladder; location of staining on vaginal swabs helps localise the fistula
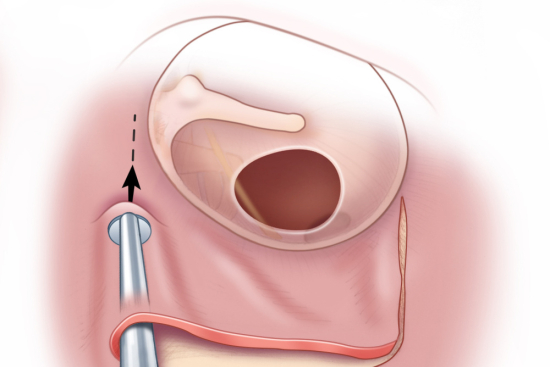
- 3. Cystoscopy — direct visualisation of the fistula opening inside the bladder; assesses size, location, distance from ureteric orifices
- 4. Intravenous urography (IVU) or CT urogram — essential for UVF diagnosis; assesses ureteric anatomy and obstruction
- 5. MRI pelvis — superior soft-tissue characterisation for complex, recurrent, or radiation-related fistulas
- 6. Retrograde pyelogram — if ureteric injury is suspected
- 7. Vaginoscopy — in selected cases


Surgical Repair of Genitourinary Fistula
Timing of Repair
The optimal timing of fistula repair is a subject of debate. Traditional teaching recommended waiting 3–6 months after diagnosis (and at least 3 months after surgery or delivery) to allow inflammation to subside, tissue oedema to resolve, and local blood supply to recover — creating better tissue for repair. More contemporary evidence supports earlier repair (within 3–4 months, or even earlier for selected post-surgical fistulas without significant tissue damage) without compromising outcomes.
Surgical Approaches
Vaginal approach — the preferred approach for most simple VVFs. A vaginal incision is made, the fistula tract is excised, healthy tissue margins are freshened, and the bladder wall is closed in layers with absorbable sutures followed by vaginal closure. A Martius flap (labial fat pad) is interposed between the layers to provide additional blood supply and prevent suture line overlap — reducing recurrence. The vaginal approach avoids abdominal surgery and has excellent outcomes for low-positioned fistulas.
Abdominal (transabdominal) approach — preferred for high VVFs near the ureteric orifices, complex or recurrent fistulas, radiation fistulas, associated ureteric injuries, or when simultaneous abdominal surgery is required. An omental flap is interposed between the bladder repair and the vaginal closure, providing rich blood supply. The abdominal approach allows ureteric reimplantation if required.
Laparoscopic / robotic-assisted repair — minimally invasive alternatives to open abdominal repair, offering faster recovery and less blood loss. Requires advanced laparoscopic expertise.
Ureterovaginal fistula repair — typically requires ureteric reimplantation into the bladder (ureteroneocystostomy), often with a psoas hitch or Boari flap to bridge the gap if significant ureteric length has been lost.
Post-Operative Care and Recovery
- a. Urinary catheter (Foley) remains in place for 2–3 weeks after vaginal repair and 3–4 weeks after abdominal repair — allowing the repaired tissue to heal without stress
- b. Complete pelvic rest for 3 months — no sexual intercourse, douching, or vaginal instrumentation
- c. Regular follow-up to confirm healing before catheter removal
- d. Cystogram performed before catheter removal to confirm watertight repair
- e. Success rates after first repair by experienced surgeons: 85–95% for VVF, lower for radiation fistulas
- f. Second repair attempts have lower success rates — emphasising the importance of expert first repair
Frequently Asked Questions — Genitourinary Fistula Hyderabad
Why Choose SurgiPartner for Genitourinary Fistula Repair?
Choosing SurgiPartner means choosing expert surgical care with dignity, privacy, and compassion.
01.
Experienced Reconstructive Surgeons
Our surgeons have extensive experience managing complex genitourinary fistula cases with high success rates.
02.
Advanced Transplant Infrastructure
We use modern surgical methods that reduce tissue damage, promote faster healing, and lower recurrence risk.
03.
Comprehensive Transplant Care
Each repair strategy is tailored to fistula type, severity, and patient health for optimal outcomes.
04.
Long-Term Follow-Up & Support
We provide structured post-operative care, follow-ups, and guidance to ensure lasting relief and confidence.
Book Your Consultation
We provide structured post-operative care, follow-ups, and guidance to ensure lasting relief and confidence.
Restoring health and dignity — that’s the SurgiPartner promise.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.