Diabetic Retinopathy Treatment in Hyderabad
Diabetic retinopathy is the leading cause of preventable blindness among working-age adults in India — and Hyderabad, with its large diabetic population, faces this challenge acutely. If you have diabetes, regular retinal screening is not optional — it is essential. SurgiPartner connects diabetic patients in Hyderabad with expert retinal specialists for comprehensive screening, monitoring, and treatment at all stages of the disease.


What Is Diabetic Retinopathy?
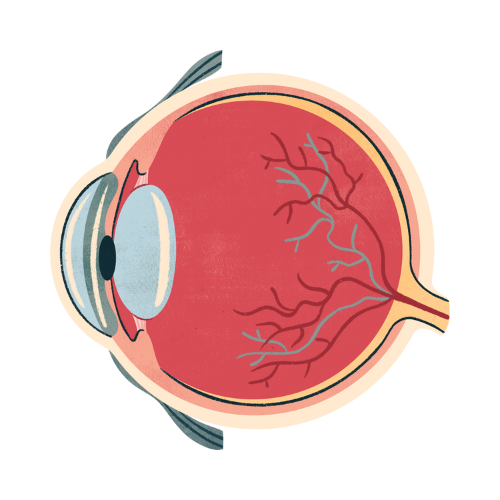
Diabetic retinopathy is a diabetes-related complication that damages the small blood vessels supplying the retina — the light-sensitive tissue at the back of the eye. Persistently elevated blood glucose levels cause these blood vessels to weaken, leak, swell, or grow abnormally, progressively impairing vision. Without treatment, advanced diabetic retinopathy leads to severe, irreversible vision loss and blindness.
In India, approximately 18% of diabetic patients have some form of diabetic retinopathy — and with over 77 million Indians living with diabetes, this represents an enormous burden of preventable vision loss. The tragedy is that diabetic retinopathy rarely causes symptoms in its early, treatable stages. By the time a diabetic patient notices vision changes, significant irreversible damage may already have occurred.
The most important message for every diabetic patient: annual retinal screening saves sight. Diabetic retinopathy detected early is highly treatable. The same disease detected late — when symptoms appear — is often impossible to fully reverse.
Stages of Diabetic Retinopathy — From Early to Advanced
Stage 1: Mild Non-Proliferative Diabetic Retinopathy (NPDR)
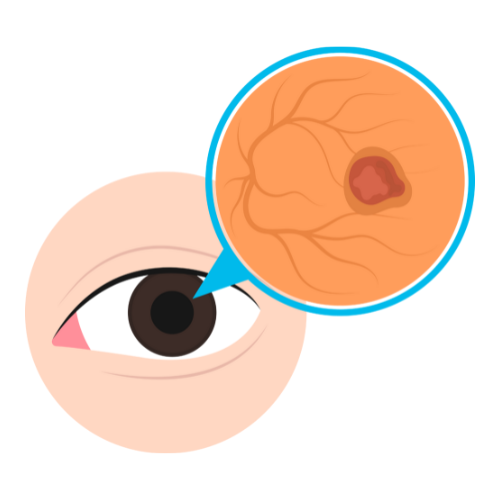
Small microaneurysms (tiny balloon-like bulges in blood vessel walls) appear in the retinal capillaries. These are the earliest detectable sign of diabetic retinopathy, visible only on retinal examination with dilated pupils or fundus photography. There are no symptoms at this stage. Treatment: optimise blood sugar, blood pressure, and cholesterol control; annual monitoring.
Stage 2: Moderate NPDR
More extensive microaneurysms, dot and blot haemorrhages (small blood leaks), hard exudates (protein and lipid deposits), and cotton wool spots (areas of ischaemia — reduced blood flow) develop. Vision may still be normal. Diabetic macular oedema (DME) can develop at any NPDR stage when fluid accumulates in the macula, causing central vision blurring. Treatment: intensive monitoring every 3–6 months; treat DME if present.
Stage 3: Severe NPDR
Extensive haemorrhages and microaneurysms in all four retinal quadrants, venous beading, and intraretinal microvascular abnormalities (IRMA). A significant proportion of blood vessels feeding the retina are occluded. This stage carries a high risk of progressing to proliferative retinopathy within 12 months. Urgent treatment is required.
Stage 4: Proliferative Diabetic Retinopathy (PDR)
The most advanced and dangerous stage. In response to widespread retinal ischaemia, the eye releases growth factors (VEGF) that stimulate abnormal new blood vessel formation (neovascularisation) on the retinal surface, optic disc, and iris. These new vessels are fragile and bleed easily — causing vitreous haemorrhage (sudden severe vision loss), tractional retinal detachment, and neovascular glaucoma. PDR requires urgent treatment.
Diabetic Macular Oedema (DMO) — The Most Common Cause of Vision Loss
Diabetic macular oedema occurs when fluid leaks from damaged capillaries into the macula — the central part of the retina responsible for reading, driving, and facial recognition. DMO can occur at any stage of diabetic retinopathy and is the most common cause of vision loss in diabetic patients. It presents as blurring or distortion of central vision, difficulty reading, and colours appearing washed out. OCT (optical coherence tomography) is used to measure macular thickness and monitor treatment response.
Diabetic Retinopathy Treatment Options
1. Systemic Control — The Foundation of All Treatment
No retinal treatment is as effective as preventing disease progression through tight metabolic control. Target HbA1c below 7%, blood pressure below 130/80 mmHg, and LDL cholesterol below 100 mg/dL. Smoking cessation is strongly advised. These systemic measures slow retinopathy progression more effectively than any single retinal intervention. SurgiPartner works closely with diabetologists to coordinate comprehensive care.
2. Anti-VEGF Injections (Intravitreal Injections)
Anti-VEGF (anti-vascular endothelial growth factor) agents — bevacizumab (Avastin), ranibizumab (Lucentis), or aflibercept (Eylea) — are injected into the vitreous cavity to suppress the abnormal blood vessel growth factor driving PDR and to reduce macular oedema in DMO. Anti-VEGF is now the first-line treatment for centre-involving DMO and proliferative retinopathy. The injection is a quick, painless outpatient procedure performed under topical anaesthesia. Multiple injections at 4–8 weekly intervals are typically required.
3. Laser Photocoagulation
Focal/grid laser treats DMO by sealing leaking microaneurysms and treating areas of oedema in the macular area. It reduces vision loss rather than improving it and has largely been replaced by anti-VEGF as first-line DMO treatment.
Panretinal photocoagulation (PRP) applies 1,200–1,600 laser burns to the peripheral retina, destroying ischaemic tissue that drives VEGF production. This causes neovascularisation to regress in 90% of PDR cases. PRP is the traditional first-line treatment for high-risk PDR and is still widely used alongside anti-VEGF.
4. Vitrectomy Surgery
Surgical vitrectomy is required for complications of advanced PDR that cannot be treated with laser or anti-VEGF alone:
- a. Non-clearing vitreous haemorrhage — blood in the vitreous that obscures vision and fails to clear spontaneously over 1–3 months
- b. Tractional retinal detachment — fibrovascular membranes pulling the retina away from the RPE
- c. Combined tractional and rhegmatogenous retinal detachment
- d. Macular tractional oedema — refractory DMO with epiretinal membrane
Diabetic Retinopathy Screening — Who Needs It and How Often?
| Patient Group | When to Start Screening | Frequency |
|---|---|---|
| Type 1 Diabetes | 5 years after diagnosis (or at puberty) | Annually, more frequently if retinopathy present |
| Type 2 Diabetes | At diagnosis | Annually — may already be present at diagnosis |
| Gestational Diabetes / Pregnancy | At first prenatal visit | Every trimester; within 3 months postpartum |
| Poor glycaemic control (HbA1c >9%) | Immediately | Every 3–6 months |
| Visual symptoms present | Immediately | Urgent — do not delay |
Frequently Asked Questions — Diabetic Retinopathy Hyderabad
Why Choose SurgiPartner?
Choosing SurgiPartner means trusting your vision with specialists who understand the complexity of diabetic eye disease.
01.
Expert Retinal Specialists
Our vitreoretinal surgeons have extensive experience managing mild to advanced diabetic retinopathy cases.
02.
Advanced Retinal Diagnostics
We use OCT scans, fundus photography, and angiography for accurate disease staging.
03.
Comprehensive Treatment Options
From injections and laser therapy to advanced vitrectomy surgery, all treatments are available under one roof.
04.
Long-Term Monitoring & Care
Diabetic retinopathy requires ongoing follow-up, and we provide structured, continuous care plans.
Book Your Consultation
Protect your vision from diabetes-related damage with SurgiPartner advanced diabetic retinopathy treatment. Early care makes a life-changing difference.
Early detection. Advanced care. Lifelong vision protection.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.