Say Goodbye to Discomfort with SurgiPartner Advanced Varicocele Treatment
Life Restored. Confidence Renewed. Comfort Reclaimed.
Varicocele Treatment in Hyderabad — Expert Microsurgical Varicocelectomy
Varicocele is the most common surgically correctable cause of male infertility — yet an estimated 35–40% of men with fertility concerns who have a varicocele remain untreated because the condition is frequently misunderstood, undiagnosed, or dismissed as harmless. The truth is that for men experiencing scrotal discomfort, testicular heaviness, reduced testosterone, or difficulty conceiving, varicocele treatment is one of the highest-impact interventions available in modern urology. SurgiPartner connects patients across Hyderabad with expert urologists and andrologists for precise, minimally invasive varicocele surgery — including microsurgical varicocelectomy (the global gold standard), laparoscopic varicocelectomy, and percutaneous varicocele embolization — with comprehensive post-operative monitoring and fertility follow-up. Insurance support available.
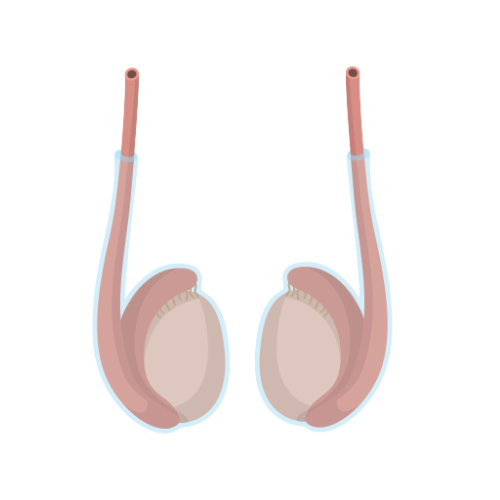
What Is Varicocele?
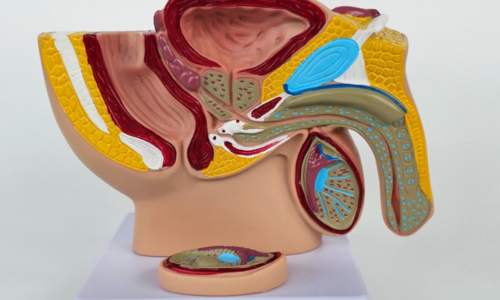
A varicocele is an abnormal enlargement and dilation of the pampiniform plexus — the network of veins that drains deoxygenated blood from the testis and epididymis within the spermatic cord. It is the male equivalent of varicose veins in the legs, occurring when the one-way valves within the testicular veins malfunction, allowing blood to pool and flow backward (retrograde) rather than draining efficiently toward the heart. This pooling of venous blood raises scrotal temperature, impairs blood flow to the testis, and creates an environment of oxidative stress and hormonal disruption that progressively damages sperm production.
Varicocele is found in 15–20% of all adult males and in 35–40% of men presenting for primary infertility evaluation. It is the single most common reversible cause of male factor infertility. It occurs predominantly on the left side (90% of cases) due to the anatomy of the left internal spermatic vein, which drains at a 90-degree angle into the left renal vein — creating higher hydrostatic pressure than the right-sided drainage. Bilateral varicocele (both sides) occurs in 10–15% of cases.
Grades of Varicocele — Clinical Classification
Varicocele severity is graded using the WHO/Dubin–Amelar clinical grading system based on clinical palpation and Doppler ultrasound findings:
Grade I — Subclinical
Detectable only by Doppler ultrasound or during Valsalva maneuver. Not palpable. Often monitored; surgery considered if semen parameters deteriorate.
Grade II — Moderate
Palpable on standing but not visible. Confirmed by scrotal Doppler. Surgery recommended when associated with infertility, pain, or testicular volume asymmetry.
Grade III — Severe
Visible through scrotal skin without palpation — "bag of worms" appearance. Almost always symptomatic. Surgery strongly recommended.
Causes of Varicocele — Why Do Testicular Veins Dilate?
The fundamental cause of varicocele is failure of the venous valves within the internal spermatic vein — the valves that normally prevent retrograde (backward) blood flow from the renal vein toward the testis. When these valves are absent or incompetent, blood flows backward under gravitational pressure, causing progressive distension of the pampiniform plexus. Several anatomical and physiological factors contribute:
- Left-sided anatomical predisposition: The left spermatic vein drains at a 90-degree angle into the left renal vein — creating higher hydrostatic back-pressure than the right spermatic vein (which drains at an acute angle into the inferior vena cava)
- Absent or incompetent venous valves: The primary intrinsic defect — found in the majority of varicocele cases
- Increased abdominal pressure: Prolonged standing, heavy lifting, chronic constipation, and occupations requiring sustained upright posture all increase intraabdominal venous pressure and exacerbate venous pooling
- Rapid growth spurts during puberty: The majority of varicoceles develop during adolescence (ages 12–18) when rapid body growth increases blood flow demands without corresponding vein wall maturation
- Valsalva-induced reflux: Activities involving breath-holding and increased intraabdominal pressure (heavy lifting, straining) temporarily worsen varicocele symptoms by increasing venous reflux
Symptoms of Varicocele — When to See a Doctor
Many varicoceles — particularly Grade I — are asymptomatic and discovered incidentally during fertility evaluation or routine physical examination. However, clinically significant varicoceles (Grade II–III) cause recognisable symptoms that progressively worsen with time and standing:
- Dull, aching scrotal pain — the most common complaint. Described as a dragging or heaviness sensation, typically worsening after prolonged standing, physical activity, or at the end of the day, and relieving when lying down
- Testicular heaviness or discomfort — a persistent feeling of weight in the scrotum, particularly noticeable after exercise
- Visible, tortuous veins — the classic “bag of worms” appearance in Grade III varicoceles, most visible when standing
- Testicular size asymmetry — the affected testis (usually left) is smaller than the opposite side due to impaired growth or progressive atrophy from poor venous drainage
- Abnormal semen analysis — reduced sperm count (oligospermia), poor sperm motility (asthenospermia), or abnormal sperm morphology (teratospermia) discovered during fertility investigation
- Low testosterone — varicocele progressively damages the Leydig cells responsible for testosterone production, causing low serum testosterone, reduced libido, and fatigue
- Infertility — difficulty conceiving after 12 months of unprotected intercourse, where semen analysis reveals male factor contribution
How Does Varicocele Cause Male Infertility? — The Mechanism
Varicocele impairs male fertility through multiple concurrent mechanisms — understanding these explains why treatment produces measurable improvements in sperm parameters:
1. Elevated Testicular Temperature
The scrotum normally maintains the testes at 2–4°C below core body temperature — essential for optimal spermatogenesis (sperm production). Pooled venous blood in a varicocele carries heat from the body into the scrotum, raising testicular temperature. Even a 1°C increase in testicular temperature significantly impairs sperm production, motility, and DNA integrity. This is the most clinically significant mechanism linking varicocele to infertility.
2. Oxidative Stress
Venous stasis and poor oxygenation within varicocele-affected vessels generate reactive oxygen species (ROS) — molecules that damage sperm cell membranes, proteins, and DNA. Elevated seminal oxidative stress markers (malondialdehyde, 8-hydroxydeoxyguanosine) are consistently found in men with clinically significant varicoceles and often normalise after successful treatment.
3. Reflux of Adrenal and Renal Metabolites
The retrograde blood flow from the left renal vein carries adrenal hormones (particularly cortisol and catecholamines) and other metabolites directly to the testicular parenchyma — disrupting the delicate hormonal environment essential for Leydig cell function and spermatogenesis.
4. Impaired Testicular Blood Flow and Hypoxia
Venous congestion reduces arterial inflow to the testis, creating relative ischaemia (oxygen deprivation) that impairs both germ cell and Sertoli cell function. Sertoli cells are the “nurse cells” of spermatogenesis — their impairment directly reduces sperm production efficiency.
5. Progressive Testicular Atrophy
Long-standing, untreated varicocele causes progressive shrinkage of the affected testis from cumulative ischaemic and thermal damage. Testicular volume directly correlates with spermatogenic capacity. Early treatment prevents irreversible atrophy.
Diagnosis of Varicocele — What to Expect at SurgiPartner
| Investigation | What It Assesses | Why It Matters |
|---|---|---|
|
Clinical Examination
(Valsalva Maneuver) | Physical palpation of spermatic cord in standing position during bearing-down effort | Grades varicocele clinically; confirms palpability; essential first step |
| Scrotal Doppler Ultrasound | Real-time colour Doppler assessment of pampiniform plexus vein diameter and reflux during Valsalva | Gold standard for diagnosis and grading; detects subclinical varicocele; measures testicular volume |
|
Semen Analysis
(×2 samples, 2–3 weeks apart) | Sperm count, motility, morphology, volume, pH, WBC count | Quantifies impact on fertility; provides pre-treatment baseline for post-surgical comparison |
| Serum Testosterone + FSH + LH | Hormonal function of Leydig cells and hypothalamic-pituitary axis | Assesses severity of endocrine impact; guides prognosis |
| Sperm DNA Fragmentation Index (DFI) | Percentage of sperm with damaged nuclear DNA | High DFI (>15%) from oxidative stress predicts poor ART outcomes; normalises after varicocelectomy in many cases |
|
Testicular Biopsy
(selected cases) | Histological assessment of spermatogenesis | Reserved for azoospermic patients to assess if sperm retrieval is possible for ICSI |
Varicocele Treatment Options in Hyderabad — Complete Guide
Varicocelectomy is the most evidence-based intervention in male infertility treatment. Meta-analyses of over 30 randomised controlled trials consistently demonstrate meaningful improvements in semen parameters and natural conception rates following treatment of clinically significant varicoceles:
- Sperm count improvement: Average increase of 9–12 million/mL in total sperm count post-varicocelectomy
- Sperm motility improvement: Average increase of 10–14% in total motile sperm
- Natural pregnancy rate: 30–50% of couples conceive naturally within 12 months of successful varicocelectomy in appropriately selected candidates
- Improvement timeline: Spermatogenesis takes 70–90 days (one cycle). Allow two complete cycles (3–6 months) before assessing post-treatment semen analysis
- Sperm DNA fragmentation: DFI typically reduces significantly by 6 months post-treatment, improving ART (IVF/ICSI) outcomes in couples needing assisted reproduction
- Testosterone improvement: Serum testosterone increases by an average of 100–200 ng/dL post-varicocelectomy in men with pre-operative hypogonadism
- Azoospermia: 20–55% of azoospermic men with varicocele develop measurable sperm in the ejaculate after varicocelectomy — potentially avoiding surgical sperm retrieval for IVF
Varicocele Treatment Comparison Table
| Factor | Microsurgical | Laparoscopic | Embolization |
|---|---|---|---|
| Anaesthesia | Local / General | General | Local + sedation |
| Incision | 2.5cm subinguinal | 3 ports (5–12mm) | None — catheter via vein |
| Recurrence | Under 1% | 4–10% | 10–15% |
| Hydrocele risk | Under 1% | 10–15% | Less than 1% |
| Return to work | 5–7 days | 3–5 days | 1–3 days |
| Bilateral treatment | Two incisions | One session | One session |
| Success (semen) | 50–70% | 45–60% | 45–55% |
| Recommended by EAU/AUA? | Yes — Gold Standard | Yes (selected) | Yes (selected) |
| Insurance Coverage | Most policies | Most policies | Selected policies |
Varicocele and Fertility — What Improvement Can You Expect?
Varicocelectomy is the most evidence-based intervention in male infertility treatment. Meta-analyses of over 30 randomised controlled trials consistently demonstrate meaningful improvements in semen parameters and natural conception rates following treatment of clinically significant varicoceles:
- Sperm count improvement: Average increase of 9–12 million/mL in total sperm count post-varicocelectomy
- Sperm motility improvement: Average increase of 10–14% in total motile sperm
- Natural pregnancy rate: 30–50% of couples conceive naturally within 12 months of successful varicocelectomy in appropriately selected candidates
- Improvement timeline: Spermatogenesis takes 70–90 days (one cycle). Allow two complete cycles (3–6 months) before assessing post-treatment semen analysis
- Sperm DNA fragmentation: DFI typically reduces significantly by 6 months post-treatment, improving ART (IVF/ICSI) outcomes in couples needing assisted reproduction
- Testosterone improvement: Serum testosterone increases by an average of 100–200 ng/dL post-varicocelectomy in men with pre-operative hypogonadism
- Azoospermia: 20–55% of azoospermic men with varicocele develop measurable sperm in the ejaculate after varicocelectomy — potentially avoiding surgical sperm retrieval for IVF
Varicocele Surgery Recovery — What to Expect
| Timeline | Microsurgical | Laparoscopic | Embolization |
|---|---|---|---|
| Day 1 | Mild scrotal discomfort; ice pack; prescribed analgesics; go home same day or after 1 night | Mild port site soreness; go home after 1 night | Mild groin ache at catheter entry site; go home same day |
| Days 2–5 | Scrotal swelling and bruising — normal and expected | Port site discomfort reducing | Return to normal activity Day 2–3 |
| Week 1 | Return to desk work; wear scrotal support at all times | Return to desk work; light activity | Full normal activity resumed |
| Week 2–3 | Light exercise resumes; sutures dissolving or removed | Most activities resumed | Full activity including exercise |
| Week 4–6 | Return to exercise, sexual activity, and manual work | Full activity | — |
| Month 3 + 6 | Semen analysis at 3 and 6 months — the critical post-treatment checkpoints | Same | Doppler assessment + semen analysis |
Why Choose SurgiPartner?
At SurgiPartner, we offer precision-based, minimally invasive treatments for Varicocele, a common condition that affects male fertility and comfort. Our advanced surgical and non-surgical techniques ensure lasting relief, improved fertility, and faster recovery – all performed by experienced urologists.
01.
Expert Urologists & Andrology Specialists
Our team of specialists has extensive experience diagnosing and treating varicoceles with proven success and minimal complications.
02.
Advanced Minimally Invasive Surgery
We use laparoscopic and microsurgical varicocelectomy techniques for greater precision, less pain, and a faster return to normal activities.
03.
Improved Fertility Outcomes
Our treatments focus not just on pain relief but also on enhancing sperm quality and fertility potential for long-term benefits.
04.
Quick & Painless Recovery
With our advanced approach, most patients experience minimal discomfort and resume daily life within a few days.
Book Your Consultation
Take the first step toward a healthier, pain-free life with SurgiPartner advanced Varicocele treatment. Our team ensures you receive accurate diagnosis, safe care, and the best possible outcomes — all with minimal downtime.
Relief and recovery — delivered with precision and care at SurgiPartner.
What Our Patients Say

Posted onTrustindex verifies that the original source of the review is Google. I am thoroughly impressed with the SurgiPartner model, which delivers integrated, end-to-end patient support across the healthcare continuum—from initial consultations to treatment and surgical interventions, where necessary. I recently availed their Care Buddy service for a consultation, and the experience was highly seamless, efficient, and professionally managed. The structured Care Buddy support, combined with well-aligned financial assistance processes, significantly enhances the overall patient journey. This holistic and patient-centric approach effectively streamlines access to quality healthcare, making it more efficient and convenient in today’s dynamic environment.Posted onTrustindex verifies that the original source of the review is Google. I’m really impressed with the SurgiPartner concept. They provide end-to-end patient support—from doctor consultations to treatment and even surgery when required. I personally used their Care Buddy service for a consultation, and it was a smooth and positive experience. The Care Buddy assistance, along with support in financial processes, makes healthcare much more convenient, especially in today’s fast-paced lifestyle.Posted onTrustindex verifies that the original source of the review is Google. My Brother Arun Kumar and krishna from Bangalore. We are travelled to Hyderabad for LASIK surgery, and today we successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner support.Posted onTrustindex verifies that the original source of the review is Google. Really impressed with the concept of SurgiPartner. They offer complete patient support from doctor consultation to treatment and surgery if needed. I personally took a consultation through their Care buddy, and it was a great experience. The care buddy system and help with financial processes make healthcare much easier, especially in today’s busy world.Posted onTrustindex verifies that the original source of the review is Google. My name is Arun Kumar and I am from Bangalore. I traveled to Hyderabad for LASIK surgery, and today I successfully underwent the procedure at American Laser Eye Hospital. The surgery went very smoothly and I am feeling very good after the procedure. The hospital environment is very clean and well maintained. All the staff and doctors are very polite, supportive, and professional. A special thanks to SurgiPartner CareBuddy for guiding and helping me throughout the entire process. From the beginning till the end of the day, they were with us at every step and provided excellent support. Overall, I had a very good experience and I highly recommend American Laser Eye Hospital for LASIK surgery with SurgiPartner supportPosted onTrustindex verifies that the original source of the review is Google. Thank you for the support and service provided by SurgiPartner. The overall experience was smooth and the team was very helpful.Posted onTrustindex verifies that the original source of the review is Google. Staff is very good and nice receiving. They are very humble and their response is very good. Thank youPosted onTrustindex verifies that the original source of the review is Google. I want to thank Surgipartner for all the help and support during my LASIK surgery. From the beginning till the end, the team was very proactive with follow-ups and guided me clearly through every step, which made the whole experience easy and stress-free. I would especially like to appreciate CareBuddy Raju and Coordinator Anusha for their outstanding support. They were always in touch with both the hospital staff and me, helped reduce waiting time, and made sure everything went smoothly. Their care, quick responses, and constant guidance really made a big difference. Overall, I had a very positive experience and truly appreciate the support provided by Surgipartner.Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Frequently asked questions
What is a varicocele?
A varicocele is an enlargement of the veins within the scrotum, similar to varicose veins in the legs. It can cause discomfort, affect testicular health, and is a common cause of male infertility.
How do I know if I have a varicocele?
Symptoms may include a dull ache, heaviness, or visible twisted veins in the scrotum—especially after standing or physical activity. Some men are asymptomatic and discover it during a fertility check-up or physical exam.
Is varicocele a serious condition?
While not usually life-threatening, varicoceles can lead to fertility problems, testicular atrophy, and ongoing discomfort if left untreated. Early diagnosis and treatment are important for long-term reproductive and urological health.
Does varicocele affect fertility?
Yes. Varicoceles can impair sperm quality, count, and motility due to increased scrotal temperature and poor blood flow. Treating the varicocele can significantly improve fertility in many men.
What is varicocelectomy, and how is it performed?
Varicocelectomy is a minimally invasive surgical procedure where the enlarged veins are tied off to redirect blood flow to healthier veins. At SurgiPartner, this is done using a microsurgical or laparoscopic technique for high precision and quicker recovery.
Is varicocele surgery painful?
The procedure is performed under local or general anesthesia, so there’s no pain during surgery. Post-operative discomfort is usually mild and short-lived, managed with rest and medication.
How long is the recovery after varicocelectomy?
Most patients resume light activities within 2–3 days and return to full activity within 1–2 weeks. Full recovery of fertility parameters may take 3 to 6 months, depending on the individual.
Are there non-surgical treatments for varicoceles?
Surgery is the most effective long-term solution. In some cases, embolization (a non-surgical procedure done by an interventional radiologist) may be an option, but it’s less commonly performed.
Can varicoceles come back after surgery?
Recurrence is rare when the procedure is done using microsurgical techniques, which have the highest success rates. At SurgiPartner, we focus on precision and long-term results to minimize this risk.
Why choose SurgiPartner for varicocele treatment?
SurgiPartner offers expert urologists, minimally invasive techniques, and personalized recovery plans focused on both symptom relief and fertility improvement. Our compassionate care and high success rates make us a trusted name in men’s health.
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.