Get Rid of Lumps Safely with SurgiPartner Advanced Lipoma Removal
Safe, Effective, and Aesthetically Perfect Lipoma Removal
Lipoma Treatment
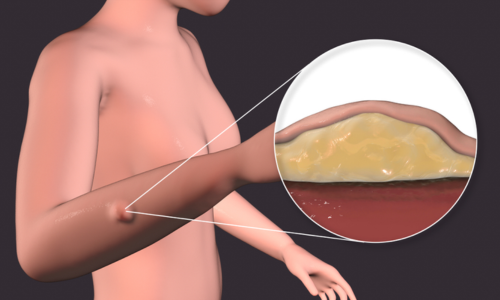
A lipoma is a benign, slow-growing tumour composed of mature adipocytes (fat cells) enclosed within a thin fibrous capsule — the most common soft tissue tumour in humans, occurring at a rate of approximately 1 per 1,000 persons per year, with a lifetime prevalence of approximately 2%. Lipomas can develop anywhere on the body where adipose tissue exists but are most frequently encountered on the neck, shoulders, upper back, trunk, upper arms, and thighs. While the vast majority are entirely harmless, certain lipomas cause discomfort, functional limitation, cosmetic distress, or diagnostic uncertainty — warranting evaluation and removal. SurgiPartner connects patients in Hyderabad with experienced plastic surgeons and general surgeons for lipoma removal as a well-planned, day-care procedure with minimal downtime.
Lipoma Treatment
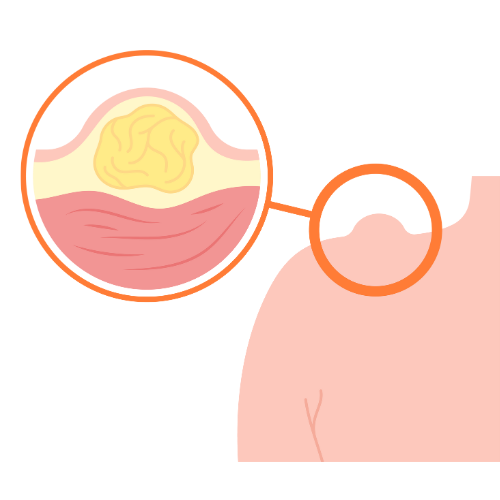
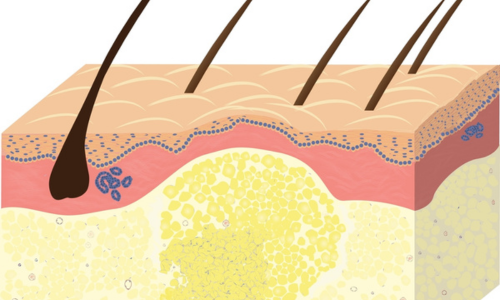
Lipomas arise from mesenchymal cells within the subcutaneous fat layer — or in some cases from deeper fat compartments between or within muscles. They are composed of differentiated, mature fat cells arranged in lobules separated by thin fibrous septa. The characteristic feature that makes lipomas distinct from malignant fatty tumours is the presence of a well-defined, complete fibrous capsule that surrounds and contains the tumour, allowing surgical enucleation (shelling out) as a complete unit.
Clinically, a subcutaneous lipoma is a soft, doughy, lobulated lump beneath the skin surface that is: mobile (slides freely under the overlying skin when pressed from side to side); non-tender in most cases (except angiolipomas); compressible; usually oval or round; and grows very slowly over months to years. The overlying skin is completely normal — unchanged in colour, texture, or temperature. Lipomas do not fluctuate (unlike cysts), are not transilluminable, and do not reduce in size.
Complete Classification of Lipoma Types
By Composition
| Type | Composition | Key Clinical Features | Treatment Consideration |
|---|---|---|---|
| Simple lipoma | Mature fat cells with thin capsule | Most common; soft; non-tender; slow growth; single lesion | Standard excision or minimal incision technique |
| Angiolipoma | Fat cells + prominent vascular component | Often painful or tender; may be multiple; typically <3cm; forearm most common site | Excision provides permanent pain relief; all specimens sent for histopathology |
| Fibrolipoma | Fat + fibrous stroma in varying proportions | Firmer consistency than simple lipoma; less compressible; can be confused with other lesions clinically | Requires standard excision; harder to enucleate than simple lipoma |
| Myelolipoma | Fat + haematopoietic (bone marrow-like) tissue | Most commonly adrenal; incidentally found on imaging; rarely subcutaneous | Adrenal myelolipoma managed by endocrinology/urology; subcutaneous excised with histopathology |
| Pleomorphic lipoma | Fat + giant cells with floret nuclei | Neck/shoulder area; elderly men; clinically indistinguishable from simple lipoma | Excision essential; histopathology confirms benign nature and excludes atypical lipomatous tumour |
| Spindle cell lipoma | Fat + spindle cells + ropey collagen | Neck/shoulder/back; men 50–70 years; clinically benign but requires histological diagnosis | Excision + histopathology; MDM2 mutation analysis in selected cases |
By Location – Clinical Significance
- Superficial subcutaneous lipoma — the most common; directly beneath the skin in the hypodermis; easily palpable; mobile with the skin; ideal for excision under local anaesthesia
- Deep subfascial lipoma — beneath the investing muscle fascia; less mobile; clinical distinction from sarcoma requires imaging (ultrasound or MRI); may be intermuscular or intramuscular
- Intramuscular lipoma — within the substance of a muscle (commonly vastus lateralis, trunk muscles); poorly defined margins; higher recurrence rate after excision; MRI assessment is mandatory before surgery
- Intraarticular lipoma — within a joint space; uncommon; causes joint swelling and mechanical symptoms; requires orthopaedic assessment
- Perirenal lipoma / retroperitoneal lipoma — within the perirenal fat or retroperitoneum; may grow to enormous size; managed by urology or general surgery
- Spinal lipoma — within the spinal canal or epidural space; causes neurological symptoms; managed by neurosurgery
- Parotid/neck lipoma — requires careful pre-operative imaging to identify proximity to the facial nerve and major neck vessels; excision by an experienced head and neck surgeon
Familial Multiple Lipomatosis
Familial multiple lipomatosis is a rare autosomal dominant condition in which patients develop dozens to hundreds of lipomas — typically appearing in the 3rd–4th decade and distributed on the trunk and extremities while sparing the hands and feet. Management is selective — only lipomas causing symptoms, functional limitation, or cosmetic distress require removal. Liposuction aspiration is useful for debulking multiple lesions with a single procedure.
Lipoma Removal Techniques — Detailed Comparison
Standard Surgical Excision
Standard excision remains the gold standard for definitive lipoma removal. Under local anaesthesia (for small-medium lesions) or general anaesthesia (for large, deep, or multiple lesions), an elliptical incision is made centred over the lipoma — the length of the incision is typically equal to or slightly larger than the lipoma’s diameter to allow adequate exposure for capsular dissection. The capsule is identified and the lipoma is enucleated by blunt and sharp dissection, maintaining capsular integrity to prevent spillage and maximise completeness of removal.
The wound is closed in anatomical layers — deep tissue approximation eliminates dead space (preventing seroma formation), followed by subcutaneous sutures and skin closure. All excised lipomas are sent for histopathological examination — this is mandatory, not optional. Procedure time: 20–60 minutes depending on size and depth. Hospital stay: day-care. Return to work: 2–3 days for superficial lipomas; 5–7 days for deeper or larger lesions.
Minimal Incision Extraction Technique
For soft, superficial lipomas up to 4–5cm in diameter, a minimal incision technique uses an access port of just 1–2cm — considerably smaller than the lipoma itself. After local anaesthesia, the small incision is made directly over the lipoma; the capsule is punctured through the small incision and the lipoma’s contents are expressed by external pressure through the opening; the collapsed capsule is then retrieved through the small incision using a haemostat. This technique leaves a scar significantly smaller than the lipoma itself — ideal for cosmetically sensitive areas such as the upper arms, face, or décolletage. Specimen is still sent for histopathology.
Liposuction Aspiration
Liposuction (tumescent technique) aspirates the lipoma contents through a 3–4mm cannula inserted through a single small stab incision. Advantages include minimal scarring (single tiny puncture), the ability to treat multiple lipomas in a single session through a small number of access points, and excellent results for large (>8cm), soft lipomas. Limitations: the fibrous capsule is not removed, resulting in a slightly higher recurrence rate than excision; specimen quality for histopathology is limited (aspirated fragments rather than whole specimen). Best used for large or multiple soft lipomas in patients who prioritise minimal scarring and have clearly benign clinical characteristics.
Steroid Injection
Intralesional triamcinolone acetonide (10–40mg) can reduce lipoma size by 30–75% through lipocyte atrophy. It does not remove the lipoma permanently — the effect is temporary and incomplete. Best suited for: very small lipomas (<1.5cm) in patients unwilling to accept any scar; as palliation for patients medically unfit for surgery; or to temporarily reduce a painful angiolipoma while awaiting definitive surgery. Not routinely recommended as primary treatment due to incomplete and temporary effect.

When Should a Lipoma Be Investigated and Removed?
Not all lipomas require intervention. Small (<3cm), stable, asymptomatic, superficial lipomas in patients who are not concerned by their presence can be safely observed with reassurance. However, the following circumstances warrant evaluation and removal:
- Rapid growth — any lipoma demonstrating rapid enlargement over weeks to months is a red flag for atypical lipomatous tumour (ALT) or liposarcoma; requires urgent imaging and biopsy
- Size ≥5cm — size alone is an independent risk factor for malignancy; lipomatous lesions ≥5cm should always be imaged (MRI preferred) and have a lower threshold for excision
- Deep location (subfascial or intramuscular) — deep-seated lipomatous tumours have a significantly higher probability of being ALT/liposarcoma than superficial lesions; all deep lipomatous tumours should be imaged with MRI and assessed by a sarcoma specialist or experienced surgeon
- Painful or tender — angiolipomas cause significant tenderness and deserve removal; any lipoma causing pain from nerve compression or pressure deserves evaluation
- Functional limitation — large lipomas restricting movement of a joint, compressing a nerve, or obstructing a body orifice require removal
- Cosmetic distress — visible lipomas on the face, neck, scalp, or décolletage that cause psychological distress and social impairment
- Diagnostic uncertainty — any lump that is firm, irregular, fixed to surrounding tissue, not clearly encapsulated on imaging, or associated with systemic symptoms (fever, weight loss) requires histopathological diagnosis
- Rapid growth — any lipoma demonstrating rapid enlargement over weeks to months is a red flag for atypical lipomatous tumour (ALT) or liposarcoma; requires urgent imaging and biopsy
- Size ≥5cm — size alone is an independent risk factor for malignancy; lipomatous lesions ≥5cm should always be imaged (MRI preferred) and have a lower threshold for excision
- Deep location (subfascial or intramuscular) — deep-seated lipomatous tumours have a significantly higher probability of being ALT/liposarcoma than superficial lesions; all deep lipomatous tumours should be imaged with MRI and assessed by a sarcoma specialist or experienced surgeon
- Painful or tender — angiolipomas cause significant tenderness and deserve removal; any lipoma causing pain from nerve compression or pressure deserves evaluation
- Functional limitation — large lipomas restricting movement of a joint, compressing a nerve, or obstructing a body orifice require removal
- Cosmetic distress — visible lipomas on the face, neck, scalp, or décolletage that cause psychological distress and social impairment
- Diagnostic uncertainty — any lump that is firm, irregular, fixed to surrounding tissue, not clearly encapsulated on imaging, or associated with systemic symptoms (fever, weight loss) requires histopathological diagnosis
Pre-operative Imaging Guidelines
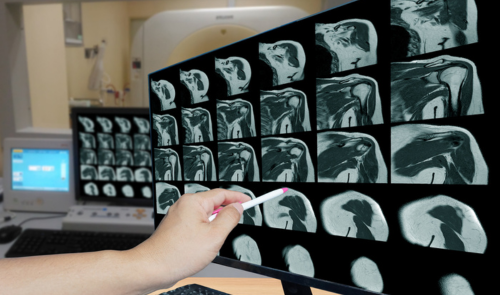
Ultrasound is the first-line imaging modality for lipomas — identifies the lesion’s location, depth (above or below fascia), dimensions, internal characteristics, and proximity to neurovascular structures. A lipoma on ultrasound shows a well-defined, echogenic, compressible lesion with no internal vascularity on Doppler assessment.
MRI with fat suppression sequences is the gold standard for: lipomas ≥5cm; deep-seated (subfascial or intramuscular) lipomas; lipomas in anatomically complex locations (neck, retroperitoneum, spinal canal); and any lipoma with atypical clinical or ultrasound features. On MRI, a benign lipoma follows fat signal on all sequences and suppresses completely on fat-suppression sequences — any non-suppressing internal component (thick septa, solid nodular areas) raises suspicion for ALT/liposarcoma and mandates specialist referral.
Post-operative Care and Expected Recovery
Wound care: The surgical wound is covered with a dry dressing for 48 hours. The wound should be kept clean and dry for the first 7 days. Showers are permitted from day 2 (pat dry gently). Baths and swimming avoided for 2 weeks. Sutures are removed at 10–14 days or dissolve on their own if absorbable sutures are used.
Activity: Most patients return to desk work within 2–3 days of simple superficial lipoma excision under local anaesthesia. Physical activity and exercise can resume at 2–3 weeks for superficial lipomas; 4–6 weeks for large or deep lipomas after general anaesthesia. Heavy lifting (over 5kg) restricted for 4 weeks in cases where the lipoma was excised from the trunk or back due to wound tension.
Scar management: Once the wound is fully healed (typically at 3–4 weeks), silicone scar gel or silicone sheets can be applied twice daily for 3–6 months to optimise scar appearance. Sun protection (SPF 50 on the scar) prevents post-inflammatory hyperpigmentation. Scar massage from week 4 helps soften and flatten the healing scar tissue.
Follow-up: Histopathology results are reviewed at 2 weeks. A follow-up assessment at 6–12 months checks for recurrence. Patients with multiple lipomas should have new lesions reassessed rather than assuming all new lumps are benign lipomas.
Frequently Asked Questions — Lipoma Treatment Hyderabad
Why Choose SurgiPartner?
At SurgiPartner, we combine advanced surgical precision with a gentle, patient-first approach to remove lipomas safely and effectively. Our laser-assisted and minimally invasive techniques ensure quick recovery and excellent cosmetic results.
01.
Expert Laparoscopic Surgeons
Our board-certified surgeons specialize in lipoma removal with minimal discomfort and a focus on aesthetic healing.
02.
Advanced Laser Technology
We use modern laser and micro-incision methods to remove lipomas safely without visible scars or tissue damage.
03.
Personalized Treatment Plans
Each lipoma is assessed carefully to provide a tailored treatment plan, ensuring both safety and long-lasting results.
04.
Pain-Free & Quick Recovery
Take the step toward smooth, lump-free skin with SurgiPartner Advanced Lipoma Removal. Our expert doctors ensure a safe, scar-free, and painless experience.
Book Your Consultation
Take the step toward smooth, lump-free skin with SurgiPartner Advanced Lipoma Removal. Our expert doctors ensure a safe, scar-free, and painless experience.
Precision, comfort, and care — the SurgiPartner way.
Smooth Recovery, Scar-Free Results Lipoma Removal Stories
Experience how our painless & bloodless laser lipoma removal helped patients achieve quick healing, clear skin, and complete comfort — with zero stitches and minimal downtime.
“I had a lipoma on my arm for years and finally decided to get it removed. The laser procedure was totally painless and bloodless, and the scar healed beautifully.”
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.