Minimally Invasive Treatment • Quick Healing • Low Risk of Recurrence
Safe & Complete Sebaceous Cyst Removal with SurgiPartner Advanced Surgical Care
Sebaceous Cyst Removal in Hyderabad — Minimal Incision Excision, Day-Care
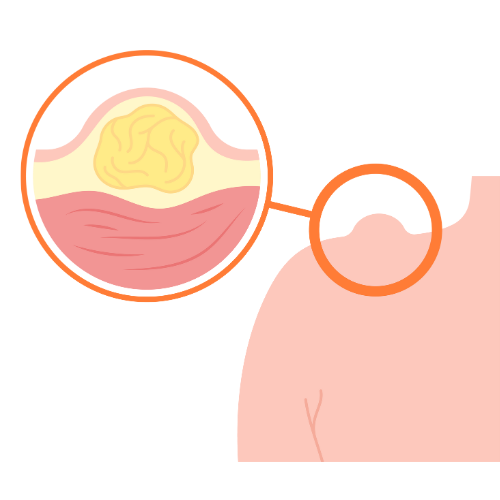
A sebaceous cyst (more accurately called an epidermoid cyst or pilar cyst, depending on location) is a slow-growing, non-cancerous, keratin-filled cyst derived from the hair follicle infundibulum or sebaceous gland. They appear as smooth, round, firm lumps beneath the skin — most commonly on the scalp, face, neck, back, and chest. While harmless, they may become infected, enlarge progressively, or cause cosmetic concern — warranting removal. SurgiPartner connects patients in Hyderabad with dermatologists and plastic surgeons for same-day cyst removal.


Symptoms & Characteristics
- Smooth, round, firm lump beneath the skin — moves freely under the skin when pressed
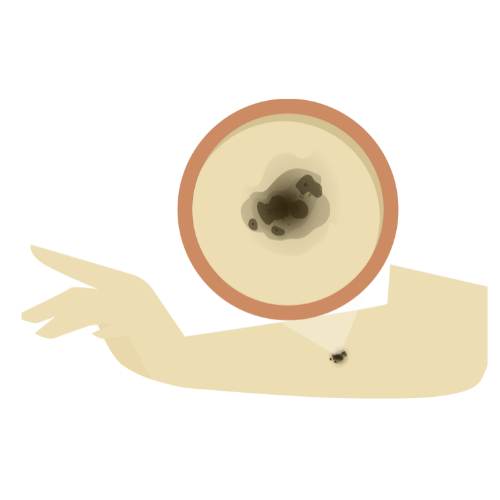
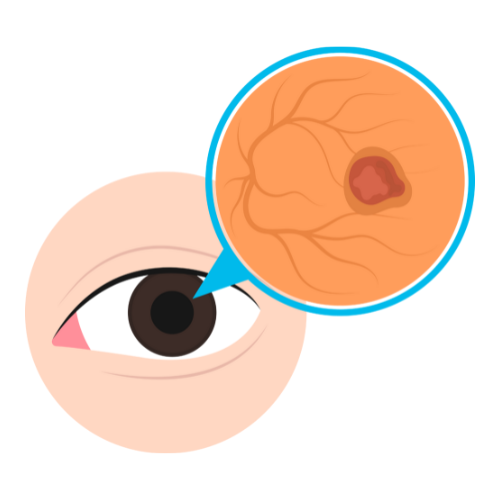
- Central punctum (dark dot) often visible — the blocked follicular opening; its presence confirms the diagnosis clinically
- Slow-growing; may remain stable for years
- Cheesy white or yellowish keratin material inside — has a characteristic unpleasant odour if it ruptures
- Infected sebaceous cyst — suddenly becomes red, hot, tender, and rapidly enlarging; may spontaneously discharge; requires drainage before definitive excision


Symptoms & Characteristics
Minimal Excision Technique (Preferred for Uninfected Cysts)
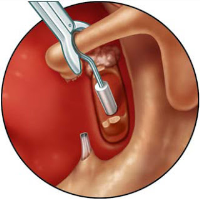
A 2–4mm punch biopsy tool creates a small circular opening over the punctum; the cyst contents are expressed; the capsule wall is retrieved through the small opening using a haemostat. Leaves a tiny scar — less than 5mm — that heals to near-invisible. Suitable for small to medium uninfected cysts. Fastest recovery: 2–3 days.
Standard Surgical Excision
For larger cysts, previously ruptured cysts, or those with thick adherent capsules. Elliptical excision removes the cyst and overlying punctum en bloc — the capsule must be removed completely intact to prevent recurrence. Performed under local anaesthesia. Leaves a fine linear scar proportional to cyst size.
Infected Sebaceous Cyst Management
Acute infected cyst: Incision and drainage first — antibiotics alone rarely resolve a fluctuant abscess. After 4–6 weeks, once inflammation has fully resolved, definitive excision of the capsule is performed. Attempting to excise an acutely inflamed cyst is technically very difficult and has a very high recurrence rate due to inability to define capsule margins in inflamed tissue.
Recovery and Post-Procedure Care
- Mild swelling, bruising, or tenderness around the surgical area is common for a few days
- Keep the dressing clean and dry for the first 24–48 hours
- Avoid squeezing, scratching, or touching the healing wound unnecessarily
- Prescribed antibiotics or pain medication should be taken exactly as advised
- Small wounds usually heal within 1–2 weeks depending on cyst size and location
- Sutures are generally removed within 5–10 days if non-dissolvable stitches are used
- Avoid gym workouts, swimming, or heavy sweating until the wound fully heals
- Scar appearance gradually improves over several weeks to months
- Most patients can return to work or routine activities within 1–3 days after minor excision
- Seek immediate medical attention if you notice pus discharge, severe redness, fever, excessive swelling, or persistent bleeding
Symptoms and Clinical Features of Sebaceous Cysts
- Smooth, round lump beneath the skin — typically 0.5–5cm in diameter; grows very slowly
- Central punctum — a small dark dot on the overlying skin surface, representing the blocked follicular opening; highly specific for epidermoid cyst when present
- Mobile beneath the skin — the cyst moves with the overlying skin when pressed (it is attached to the skin by the punctum and capsule) but moves independently of underlying muscle and fascia
- Non-tender when uninfected — smooth and painless; only becomes uncomfortable when it enlarges or is subjected to repeated trauma (e.g. under a bra strap or waistband)
- Characteristic cheesy contents — if the cyst ruptures spontaneously or is inadvertently squeezed, white-yellow, paste-like material with a distinctive unpleasant odour is expressed
- Ruptured cyst — when keratin contents leak into the surrounding dermis (from rupture or repeated squeezing), a severe foreign-body inflammatory reaction occurs — the area becomes acutely red, hot, swollen, and very tender, resembling an infection (though often not truly infected). This inflamed, ruptured cyst must be allowed to settle before definitive excision is planned
Symptoms and Clinical Features of Sebaceous Cysts
Standard Elliptical Excision
Under local anaesthesia, an elliptical incision encompassing the punctum and a small ellipse of overlying skin is made — always including the punctum, which is the cyst’s attachment to the skin surface. Dissection proceeds in the plane between the cyst capsule and the surrounding dermis — the correct plane is identifiable by the shiny, pearlescent surface of the intact capsule. The cyst is delivered intact by a combination of blunt and sharp dissection, maintaining capsule integrity to prevent spillage. Any spillage of keratin contents into the wound should be thoroughly irrigated with saline as contamination increases the inflammation and risk of recurrence.
The wound is closed in layers: absorbable deep dermal sutures to obliterate dead space; non-absorbable or absorbable fine sutures to close the skin. Specimen sent for histopathology. Procedure: 15–45 minutes. Day-care. Return to work: 2–3 days.
Minimal Incision (Punch Excision) Technique
For uninfected epidermoid cysts up to 4–5cm, a 3–4mm punch biopsy tool creates a circular access port directly over the punctum. The cyst contents are expressed through this small opening; using a fine curved haemostat, the collapsed capsule wall is grasped and gradually drawn out through the small port. The entire capsule is retrieved intact. The wound requires no sutures (4mm) or 1–2 sutures (if skin tenting occurs). Advantages: scar considerably shorter than the cyst diameter — ideal for cosmetically sensitive areas. Disadvantages: requires careful technique to extract the complete capsule; slightly higher recurrence if capsule fragments remain.
✅ Key surgical principle: The complete cyst capsule — every millimetre — must be removed for definitive cure. Squeezing or draining a sebaceous cyst without removing the epithelial capsule only temporarily empties it; the cyst will refill completely within weeks to months. There is no non-surgical permanent cure for sebaceous cysts. Call SurgiPartner on +91 9030053009 for a same-day assessment in Hyderabad.
Frequently Asked Questions — Sebaceous Cyst Removal Hyderabad
Why Choose SurgiPartner for Sebaceous Cyst Removal?
Choosing SurgiPartner means choosing safe, effective, and cosmetically superior treatment.
01.
Experienced General Surgeons
Specialists with extensive experience in minor skin and soft-tissue surgeries.
02.
Advanced Minimally Invasive Techniques
Small incisions, minimal tissue damage, and faster healing.
03.
Complete Cyst Excision
Removal of the entire cyst wall to significantly reduce recurrence risk.
04.
Comprehensive Post-Procedure Support
Clear aftercare guidance and follow-up to ensure smooth recovery.
Book Your Consultation
Take the first step toward relief from abdominal pain with SurgiPartner Advanced Appendectomy Surgery.
Live free from pain and discomfort that’s the SurgiPartner promise.
Sebaceous Cyst Removal – Patient Experiences
“The procedure was quick and completely painless.”
Your Personalized Path to Wellness
Follow your step-by-step guide to a successful surgery and recovery, with our expert team supporting you all the way.
Book FREE Consultation
Fill in your details and we'll call you back to confirm your slot.